In health care, there is no such thing as “normal business hours.” Babies insist on being born at 3 a.m. A car crash or bursting appendix can land a patient in the Emergency Room at noon or midnight or 5 a.m. To prevent infections, the cleanliness of hospital rooms is just as important at 4 a.m. as at 4 p.m.
So what’s a unit-based team to do? Full participation in a team’s performance improvement work from all members on all shifts can send service and quality scores soaring—while shifts left out in the cold can drag down a whole department. It’s hard enough ensuring all members of a single shift are on board.
But getting everyone onboard around the clock is a daunting challenge. Shifts that pass in the night may be oblivious to the other’s particular challenges and culture. They might not fully understand how their own work affects the other shift’s workflow. Rivalries and finger-pointing can ensue.
NIGHT OWLS IN THE LAB
As the double doors swing open, cold night air blasts into the receiving bay at the Regional Reference Laboratory in North Hollywood, California. Employees are ready, bundled up in knit scarves and hoodies. It’s 11:30 p.m. on a mid-February night, and couriers are delivering gray cooler bags filled with vials and tubes of specimens from all over Southern California. Clinics from Kern County in the north to San Diego, nearly 180 miles south, have closed for the evening. Now all of those blood tests and urine samples have to be processed and analyzed so providers can detect disease or spot the warning signs of a developing chronic condition.
At the specimen processing department, the graveyard shift is the busiest. “We’re like the mailroom,” says Leland Chan, supervisor and management co-lead. More than 10,000 specimens go to the automated chemistry department during the graveyard shift, compared with about 4,300 in the morning and nearly 9,000 at night.
Michael Aragones, the labor co-lead, likens the three shifts to gears all rotating together and powering each other forward. But not so long ago, the gears were getting jammed up.
Building resentments
Something was going on: Staff members on each shift thought the workload wasn’t being distributed equally—and they were getting the short end of the stick. Employees with different duties on the same shift felt the same way about their peers.
“There was a lot of ‘back talk’ between the shifts,” says Aragones, a lab assistant II and member of SEIU UHW. “People would say, ‘How come they are doing this or that?’ and ‘How come I have so much work?’ ”
The unit-based team was the vehicle for improving the workflow. Team members from all shifts got involved collecting, collating and analyzing data about the specimen count, hour by hour.

Riverside EVS attendant Virginia Gonzalez, a United Steelworkers Local 7600 member.
The results revealed why employees were feeling overworked: Between 2008 and 2010, the number of specimens going to bacteriology, for instance, increased from fewer than 4,000 to more than 5,000. Moreover, the time of night that most specimens arrived had changed. The lab used to see a big spike around 9:30 p.m.; now the rush came about 11 p.m. So the team adjusted the start and end time of the graveyard shift to match the flow of work coming in.
“At first, there was a lot of resistance,” Chan says, with employees worried about child care arrangements and traffic. The data, however, “gave us a better understanding of the workflow,” which let staff members see why they were being asked to make changes. “It was the UBT that helped solve that.”
“It wasn’t managers saying, ‘Well, you just have to,’ ” Aragones says. “We have to look at workflow for the whole department, not just one shift. It’s like a spider web. You pull one strand, and it affects the whole thing.”
Now that the work is flowing better, the UBT is working on new initiatives.
“The UBT makes my life easier,” says Chan. “It allows me to work more closely with the crew because we are on equal terms. Sometimes, as a manager, you don’t have all the answers. They do the work, they are the experts.”
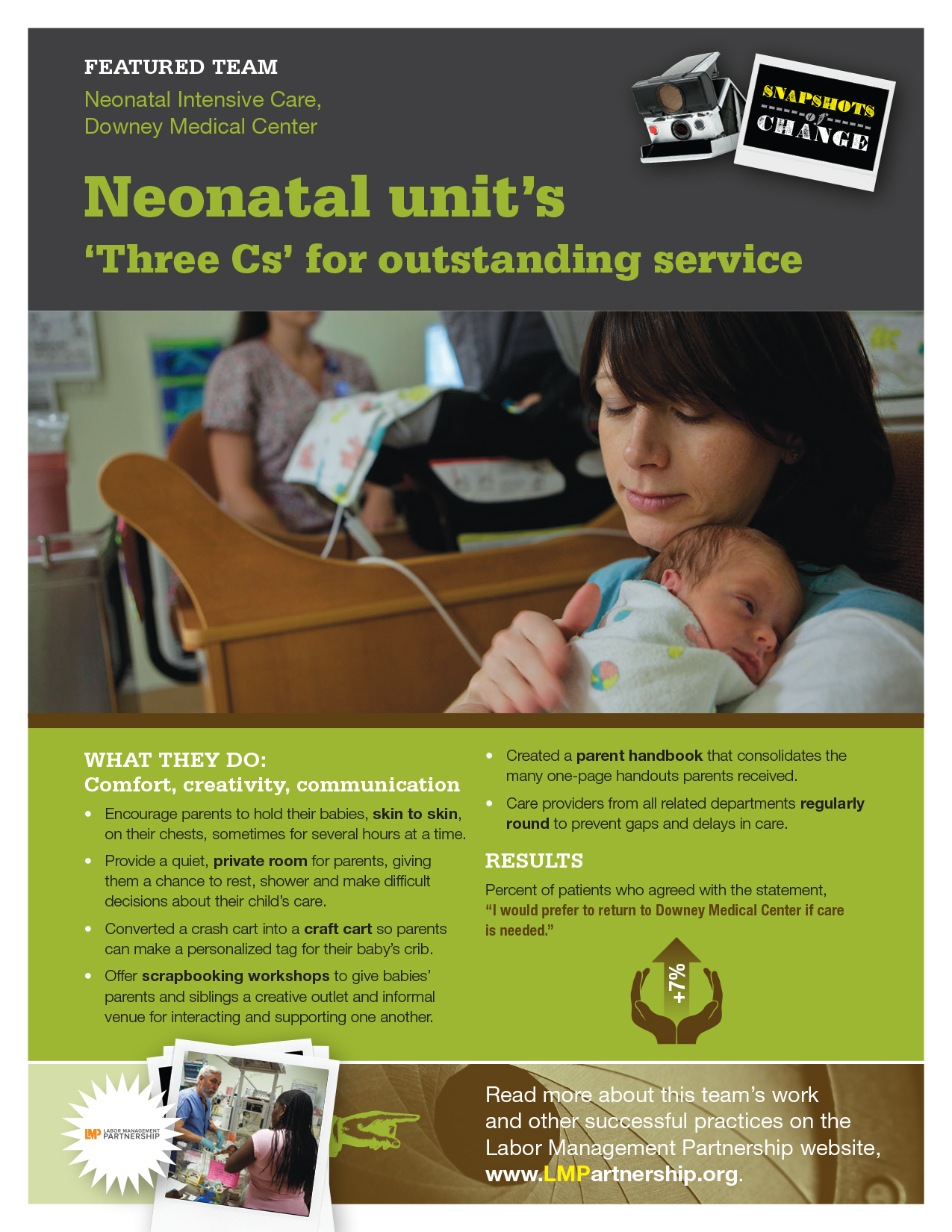
COOKING UP CAMARADERIE
It is 7:15 p.m. in the kitchen of the Downey Medical Center. “Huddddlllle!” shouts Francisco Vargas, a gentle giant of a man. The sound of his booming voice echoes off the tile floors and stainless steel work surfaces. One of about 20 SEIU UHW members working the night shift in the Food and Nutrition department, Vargas gathers the troops before they begin to wash dinner trays and deliver late meals to patients.
Assistant Department Administrator Patricia Villareal and her union partner Amelia Cervantes review new data on the team’s improvement projects, such as cooking less soup on weekends so less is wasted, and give a reminder about clocking in accurately.
The huddle ends with a team cheer—“Work hard, stay positive!”—and with that, food service kitchen worker Nancy Rudeas, an SEIU UHW member, and a colleague scurry off to prepare two late dinner trays. They double-check to see that a patient’s special request for green tea is being filled (it is).
“I love doing this,” Rudeas says, heading up on the elevator.
A few late tray deliveries have become a fact of life for the department, a consequence of abandoning set meal times in favor of a “room service” model: Patients simply make a phone call when they are ready for a meal, just like a hotel guest might.
This patient-centered innovation meant the workflow changed. Foreseeable peaks and valleys in cooking and cleaning became a less predictable, variable demand. Tasks that once had been the domain of one shift or the other “leaked” into the next shift. Tensions rose among employees as the distribution of work was thrown into flux.
“Because we have a UBT, we could sit down together and ask, ‘How can we get this resolved?’ ” says Villareal.
Together, the team experimented with adjusting start times for different jobs in the department until it settled on a mix that’s working. “The morning picks up for the night shift, and the night shift picks up for the morning,” she says.
From OK to great
The department set out to improve its customer service scores in September 2008. Though a respectable 86.7 percent of patients surveyed agreed with the statement “the people serving my meals were polite and professional,” that was nonetheless among the lowest scores in the Southern California region.
Together, the UBT members came up with a script that encourages food service workers to introduce themselves by name, ask if they can open any containers, and—most crucially—ask if there is anything else they can get for the patients. By consistently using the script, by October 2010, the score shot up to 99 percent.
Night-shift workers like Rudeas have contributed to that success. The shifts share information in huddles and bulletin boards.
“What goes on during the day, we know at night,” she says. “And what goes on at night, they know during the day.”
A SWEEPING SUCCESS
The Environmental Services department at Riverside Medical Center is continuing its winning streak: In 2010, it went 260 days without a workplace injury. The UBT received a huge banner congratulating it on the achievement, and the co-leads thought it would be nice if each team member signed it before hanging it up.
The banner remained out for a few days to make sure all staffers had a chance to sign—including the workers who come in at 11 p.m. for the graveyard shift. Only then was the banner hung up on the unit wall.
“This made a huge difference,” says Angel Pacheco, who will become the new management co-lead in May and who himself works the night shift. “This actually shows that everyone is involved and can take pride and ownership.” After all, performance metrics are measured by department, not shift, and night shift workers contributed to creating a safer workplace as much as their day shift counterparts.
The EVS team posts a flipchart sheet after every monthly UBT meeting with three to four important items of information to pass on to the rest of the staff. Each shift reviews the sheet at a daily huddle held at the beginning of each shift. The quick review of UBT business, including key performance metrics, follows the team’s stretching exercises that have helped reduce workplace injuries and won it recognition throughout KP.
The sheet hangs on the door of the supply closet, where each staff member comes when starting work to get carts, trash bags and keys to the offices they have to clean. This strategic placement ensures workers from all shifts have access to the daily UBT updates.
Face time matters
Face-to-face communication augments written communication and helps build the camaraderie that helps teams improve performance. For instance, Pacheco makes a point of visiting the night workers in the outlying medical office buildings—he drives an hour to Temecula to see one employee.
“It’s worth it,” he says. “I just take the time to reflect on things.”
Paula Cunningham, an EVS attendant and member of Steelworkers Local 7600, is one of four union members on the 6 p.m. to 2 a.m. shift responsible for passing information from the UBT’s representative group meeting to her shift colleagues.
“They trust us to deliver the information to them,” says Cunningham, whose work schedule is adjusted so she can attend representative group meetings in the early afternoon. “We talk frequently and rely heavily on huddles.” Other night shift workers also rotate into the group’s meetings.
Because he’s an on-call employee, Robert Casillas works all the shifts, so he has insights into what makes each shift unique.
The morning shift is more hectic, he says. The evening work is much calmer. More people are cleaning sections solo, but they pass one another in the hallways and share information with each other then.
“We have our communications plan, which we share with the other staff,” Casillas says. “We don’t want anyone to think we’re hiding stuff. And when the information comes from us, it’s less like a demand from management. It’s more about figuring out ideas to help us do our work.”
Sometimes, seeing the hospital at the end of the day as they do, it is night shift employees who spur the entire department into action.
The night workers noticed the hospital was running low on privacy curtains. When the ones soiled during the day were taken down, there were not enough from the laundry to replace them. Cunningham brought the information to the representative group, and the co-leads secured more curtains.
“What affects the night shift,” she says, “usually affects all of us.”