TOOLS
Understanding Sponsorship Checklist
Format:
PDF
Size:
8.5" x 11"
Intended audience:
UBT co-leads
Best used:
As a checklist for a sponsor in getting started and understanding the role.
This short animated video explains how to find and use our powerful how-to guides
Does your team want to improve service? Or clinical quality? If you don't know where to start, check out the team-tested practices on the LMP website. This short video shows you how.
Having trouble using the search function? Check out this short video to help you search like a pro!
Need to find a checklist, template or puzzle? Don't know where to start? Check out this short video to find the tools you need on the LMP website with just a few clicks.
Format:
PDF
Size:
8.5" x 11"
Intended audience:
UBT co-leads
Best used:
As a checklist for a sponsor in getting started and understanding the role.
Format:
PDF
Size:
8.5" x 11"
Intended audience:
Frontline managers; UBT sponsors and co-leads
Best used:
This table offers key tips and summarizes factors that are essential for successful UBTs.
Format:
PDF
Size:
8.5" x 11"
Intended audience:
Frontline workers, managers and physicians; UBT co-leads
Best used:
Inspire your team members to create a culture of excellence every day, everywhere.
Format:
PDF
Size:
8.5" x 11"
Intended audience:
UBT sponsors, consultants and co-leads
Best used:
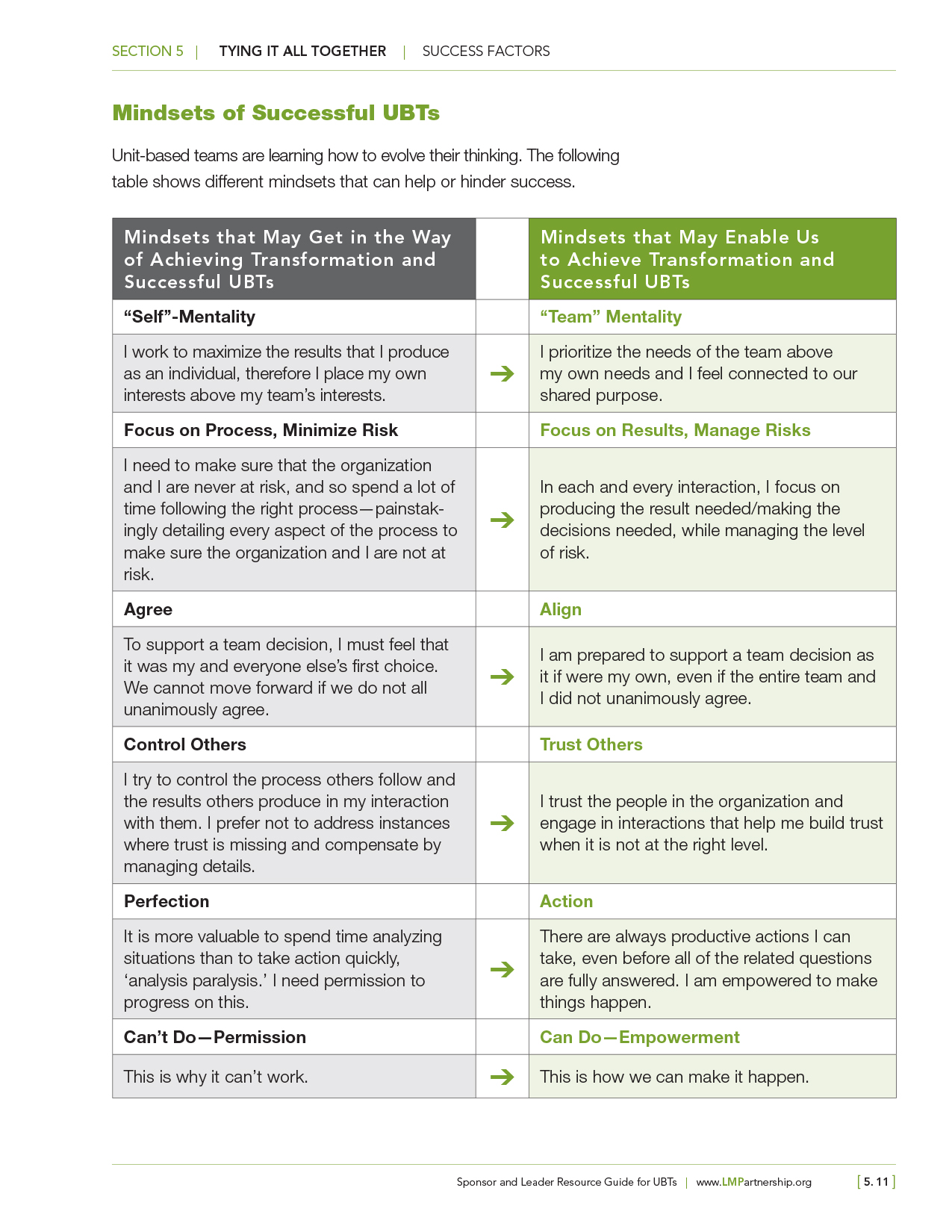
Unit-based teams can help or hinder success because of their mindset. This table lists six ways that team members learn to evolve their thinking on successful UBTs.
Format:
PDF
Size:
8.5" x 11"
Intended audience:
UBT sponsors and leaders
Best used:
This chart lays out for sponsors and leaders the difference between new, transformative mindsets that help create a team-based approach to member/patient care and traditional hierarchical thinking.
Format:
PDF
Size:
8.5" x 11"
Intended audience:
Managers and leaders
Best used:
This chart defines division of labor between management and leadership, from the beginning through the outcome of projects and changes.
The folks at the Denver Regional Pharmacy found their unit-based team to be a major improvement over the steering committee it replaced.
Team members found the committee to be unwieldy, and felt it largely bred distrust and miscommunication between union and management.
So, they regrouped.
A major problem they had encountered was the time pharmacy technicians wasted researching prescriptions that weren’t properly "batched." Often missing was the required electronic stamp from a pharmacist that tracks and closes the prescription.
Technicians spent roughly 1-4 hours a day per pharmacy tracking down misbatched prescriptions. The team aimed to cut that time by 50 percent.
"The biggest thing is if you view your situation as a failure you'll never succeed," management co-lead Luanne Petricich says. "When something is not working that's where your opportunity is. Don't be afraid to change something if it's not working."
The team modified the way pharmacists attached their electronic signature. That saved technicians hours of research time and freed them to spend more time with patients. Almost immediately the team saw a drop in the number of prescriptions that needed to be researched.
In the two pharmacies where the team instituted new batching practices, they saw a 75 percent drop in the number of prescriptions requiring research. The new protocol was introduced to 20 pharmacies in the region, and 70 percent of those saw similar gains.
This collaborative effort produced positive results as their projects improved customer service and affordability. The new UBT also gained some hard-earned trust.
Since that success, the regional team has become a model and a sponsor for smaller, pharmacy-specific UBTs launched in the region.
"I like the focus on efficiencies and waste because it ends up translating to a better work environment for employees," Petricich says. "Especially with this project, we found the technicians were doing redundant work that did not provide job satisfaction. So taking that away allowed for more time with patients, which is what many would rather be doing."
The MRI unit at Kaiser Sunnyside Medical Center had a challenge.
The department was receiving an average of 120 cases each day, but they were able to see only 71. As a result, patients were being referred outside of the Kaiser Permanente system. This drove up referral costs, inconvenienced KP members, and increased dissatisfaction.
In addition, referring patients to outside services posed a delay in getting results back to the ordering doctors. Schedulers who received the request for appointments also had a tough job—when they were not able to accommodate patients within the KP system, they had to make arrangements with outside services, which took additional time.
And finally, the patients didn’t like it.
The feedback from patients to department manager David Barry, was that they didn’t want to have to go elsewhere for services. Patients preferred to have their MRIs performed at the Sunnyside Medical Center.
The team's first step was to increase capacity to see more patients and reduce outside referrals by at least 10 per week within two weeks. To acccomplish this, they reduced the overlap in staffing and changed the schedules of two technologists, increasing their ability to see more patients.
The new staffing schedule, which didn’t infringe on union contracts, came out of a brainstorming session and was supported by staff and physicians.
After the first two technologists adjusted their schedules, a third technologist, seeing the difference it made, offered to adjust his schedule. By the end of one week, about 15 more patients were added to KP’s schedule and not referred to outside services. This resulted in a cost savings of about $7,500 per week, or about $30,000 per month.
"One of the big advantages that we have found is that we have openings for certain appointment types within a day or two, not a week or two," says labor co-lead Heather Thompson.
In addition to the work done in the UBT, a mobile scanner was added to the department. This enabled an additional 11 patients per day to be seen—or about 55 patients per week—for an additional per week savings of $30,000 in outside referral costs.
"There is a downside to that, though,” Thompson says. “Since patients are able to get the appointment so quickly, it seems as though we have a lot more short-notice cancellations and we do not have a wait list to fill them with. That is something that we will need to monitor and try to come up with a solution to."
The Mammography Department at Sunnyside Medical Center was seeing about 370 patients per week, but 25-30 percent of those appointments were running behind schedule.
Appointments ran late because information was missing from the file, additional forms were needed or the wrong test had been ordered. This cost the technologist additional time tracking down information or following up on needed documentation during the patient’s appointment, which had a cascading effect.
The unit-based team (UBT) realized that many of the issues causing delays during appointments could be handled in advance of the patient's arrival. The team came up with the idea of setting time aside every afternoon for a technologist to review the following day's orders.
"Many times patients who are coming in for an appointment are here because something has shown up on a prior screening and their anxiety and stress levels are high,” Cheryl Maize, manager of Mammography, and UBT co-lead says. “By streamlining our appointments and ensuring appointments run on time, we are hoping to allay some of that stress."
Initially, a 3-4 p.m. window was set, but as staff began to test the new process, they learned that starting the work that late in the afternoon was not ideal.
In some cases, they needed to return phone calls or required additional information, and they couldn't get everything done by the end of the day. The team pushed up the pre-work orders to a 1-2 p.m. time slot and the results improved.
In addition, the team implemented a "double-check" system at 4 p.m., so orders were again reviewed to make sure any outstanding items had arrived and everything was ready for the patient's appointment the following day.
The technologist reviewing the orders also would leave notes in the file if there was something the technologist who was seeing the patient needed to know.
Patient experience improved with the new process. Appointments were on time, and technologists were better prepared to work with their patients because the orders had been reviewed in advance.
"The implementation of the screening of orders 24 hours prior to patient arrival has allowed us to maintain our allotted appointment times and has made it easier to accommodate surprises such as late arrivals and walk-ins," Laura Wellnitz, technologist, and UBT labor co-lead says.
Eventually, a technologist was checking orders and printing out appropriate paperwork for diagnostic mammograms one day in advance of the appointments. This eliminated 10-20 minutes per appointment. As a result, most diagnostic appointments were completed in the scheduled 30 minutes, so subsequent appointments started on time.
Other staffers also preferred the new process. They decided to take turns verifying and reviewing orders, which provided a welcome break in the daily routine.
When UBT co-leads at Sunnyside Medical Center took a closer look at their patient safety assistant usage, they agreed that reducing the number of hours was a top priority.
The patient safety assistants, also known as PSAs, were certified nursing assistants and provided a key service. They were assigned to sit in a room with a patient who had dementia, was confused or at risk of a fall. They could help if the patient tried to get out of bed, remove their IV lines, or became disoriented or restless.
And patients getting out of bed is not unusual.
Some try to get out of bed because they're bored and restless or they might need to use the bathroom. Restless patients often need a change of scenery, which might mean moving the patient to the nurses' station or to a public area. There might be a need to reduce noise by closing doors at shift change to keep it quiet.
During a five-month stretch, the Sunnyside nursing unit had used 1,550 hours on PSAs. At a cost of $62,000, they wanted to bring those hours down without adversely impacting patient care.
So staff members made it a priority to talk with the patients and families to learn about the patient's interests and hobbies and offer specific activities for patients to do during their stay.
"Using the activity boxes (which contain games, crafts, videos and more) with patients has been a great way to help patients stay busy, and it makes them feel better," according to UBT labor co-chair Glenda Vosberg, RN.
The goal was to reduce PSA usage by 10 percent in four months. Knowing this was going to be a full-team effort, a mandatory in-service was scheduled and the co-leads explained the situation to the rest of the team.
They trained staff on the options to using PSAs. They provided the team with baseline data and information on the financial impact of using PSAs, and had nurses assess patients to determine whether a PSA is needed.
The results were immediate.
In a month, hours dropped from 549 to 32 without any negative impact on patient safety. Within another two months, PSA usage fell to eight hours.
"Staff were given the data and information to help them understand the impact of the situation and get their feedback on alternative options to using a PSA," says Imelda Zapata, department manager and management co-lead.
The team also enlisted the assistance of Susan Woods, the clinical nurse consultant in the hospital.
One of Woods' responsibilities was to provide consultations with patients who were assigned PSAs. She worked with the patient, family and nurse to develop a plan that best fit the needs of the patient.
Kaiser Permanente also invested in several different equipment options, including low beds, which can be put all the way down to the floor, and bed and chair alarms that let nurses know if a patient tries to get up.
The combination of equipment, changes to the environment, and activities for patients allowed the team to keep their patients safe and improve their morale while decreasing the usage of PSAs.
"Often staff is concerned about patient safety when we talk about alternatives to assigning PSAs and may be reluctant to try other options. However, literature (and our local experience) shows that having a PSA in the room does not guarantee the patient won't fall or pull out their IV lines," Woods says. "We've found that reduction of PSA usage has not negatively impacted patient safety, just as the literature suggests."