TOOLS
Crossword: All Work, No Play
Format:
PDF
Size:
8.5" x 11"
Intended audience:
Frontline employees, managers and physicians
Best used:
Unlock key words and phrases that describe factors related to stress.
This short animated video explains how to find and use our powerful how-to guides
Does your team want to improve service? Or clinical quality? If you don't know where to start, check out the team-tested practices on the LMP website. This short video shows you how.
Having trouble using the search function? Check out this short video to help you search like a pro!
Need to find a checklist, template or puzzle? Don't know where to start? Check out this short video to find the tools you need on the LMP website with just a few clicks.
Format:
PDF
Size:
8.5" x 11"
Intended audience:
Frontline employees, managers and physicians
Best used:
Unlock key words and phrases that describe factors related to stress.
Format:
PDF
Size:
8.5” x 11”
Intended audience:
Frontline employees, managers and physicians
Best used:
Use this meeting icebreaker as a fun way for getting people laughing and de-stressing.
Format:
PDF (color and black and white)
Size:
8.5” x 11”
Intended audience:
Frontline employees, managers and physicians
Best used:
Give yourself and your staff a break because attitude can be a matter of perspective. Take some down time, hit pause and reflect.
The new goal was dramatic: Reduce hospital stays to 23 hours for total joint patients.
Renee Portillo, RN, was worried.
“It was a shocker. Our staff was used to patients going home in two to three days,” says Portillo, former assistant clinical director and management co-lead of the 7 South medical-surgical team at Fontana Medical Center in Southern California.
The accelerated time frame meant that the unit’s nurses, who care for total joint patients following surgery, would have less time to prepare them for discharge. They’d also need to help choreograph care across multiple departments—Orthopedics, the operating room, Physical Therapy, Home Health—from pre-admission to discharge.
Who best to help the team through this change? The team itself.
“We used our UBT to help change the culture,” Portillo says.
“We helped our nurses be successful by having them anticipate patients’ needs and prepare them for discharge,” says Enrique Rivero, RN, a surgical nurse and UNAC/UHCP member who is the team’s union co-lead.
Fontana is among a growing number of hospitals across the United States to offer a combination of shorter hospital stays and more outpatient care for hip and knee replacement patients. The trend is driven by less-invasive surgical techniques, improved pain management and rehabilitation practices, and patients’ desire to return home as soon as possible.
“There were a lot of challenges. A lot of it had to do with bringing people together,” says Mary Hurley, MD, chief of Orthopedics, who championed the new approach. “They all had to buy in and be willing to support this in order to have a successful program.”
The new approach, which Fontana introduced in January 2014 after months of researching best practices, gets patients walking within hours of surgery and enables them to recover within the comfort of their own homes. The initiative takes advantage of Kaiser Permanente’s integrated model of care and is designed to improve clinical outcomes and reduce costly hospital stays.
Format:
PDF
Size:
8.5" x 11"
Intended audience:
UBT consultants, sponsors and co-leads
Best used:
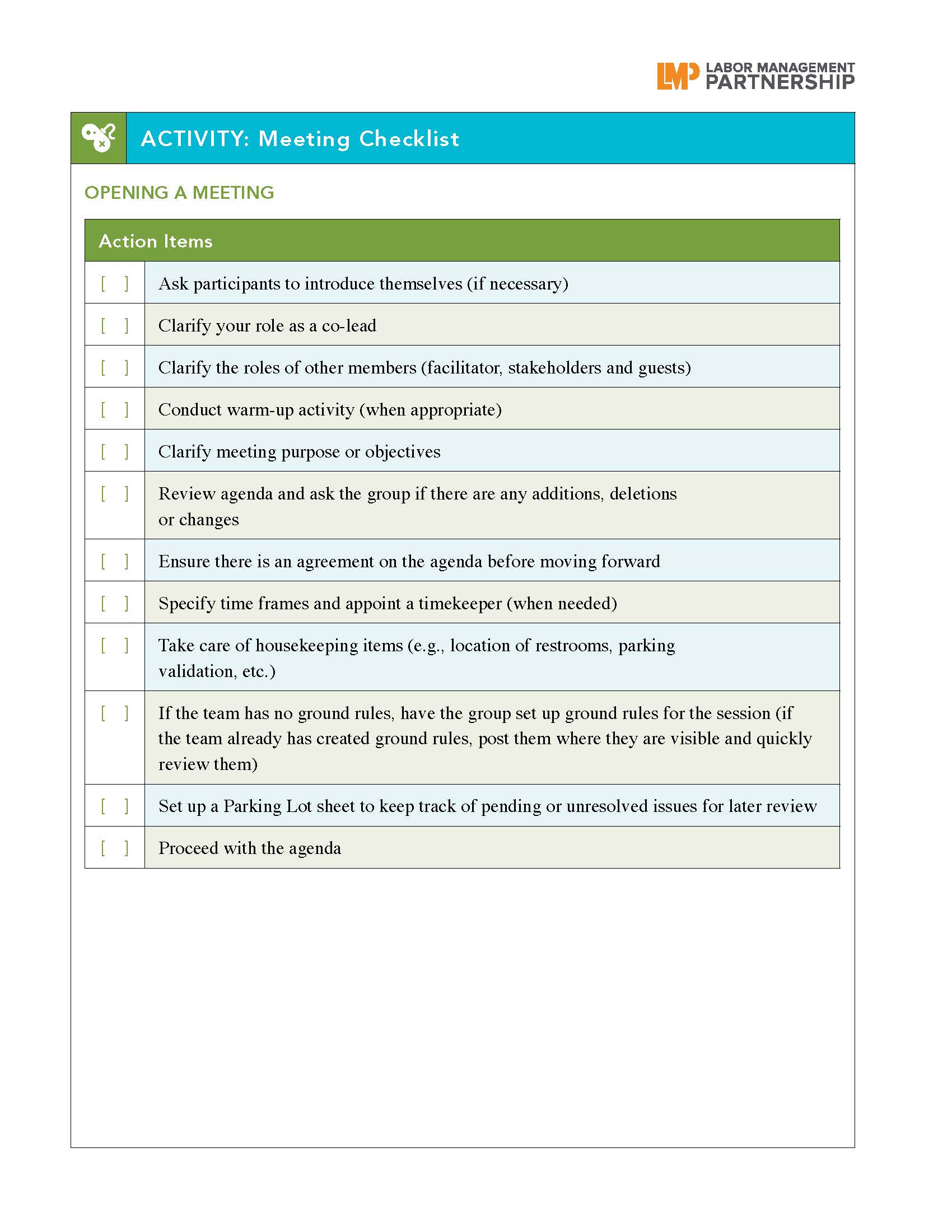
These checklists can be used as a guide to help you through opening, running and closing a meeting with your team.
On a warm fall afternoon, nearly 35 children are bouncing off the walls as they get ready to leave the classroom and head out to their elementary school’s garden. They’re all members of an after-school garden club and cooking class called Edible Olympic. It’s the brainchild of Maria Peyer, an oncology nurse and team co-lead at the Longview Kelso Medical Office in Kaiser Permanente’s Northwest region and her husband, elementary school teacher Michael Bixby.
The kids can barely contain their excitement as Bixby tries to calm them down so they can listen to the afternoon’s agenda.
“The sooner you settle down and be quiet, the quicker I can finish what I need to say and you can get outside,” he implores the class.
Quickly, the hubbub settles. Bixby goes over what needs to be done: plant blueberry bushes, dig a hole for a tree, and remove bamboo sticks. He also reviews the Garden Guidelines, which include listening with respect, walking (no running) in the garden, and asking for permission before picking anything. Then he asks, “Whose garden is it?” and gets a resounding and loud, “Ours!” as everyone heads outside to get to work.
The students attend Olympic Elementary School in Longview, Washington. They don’t have many advantages: More than 20 percent of the city’s population is below the federal poverty line, and 90 percent of the school’s students participate in the free or reduced-price lunch program. Many experience food insecurity regularly, not knowing if they’ll have enough—or any—food to eat.
There are well-documented health disparities related to low income, and these kids are at risk. Edible Olympic is helping address that vulnerability, teaching the kids about healthy food and how to prepare it, laying the foundation for good eating habits that last a lifetime. It’s an example of how partnership principles expand naturally and necessarily into the community; the new 2015 National Agreement includes commitments to jointly work on improving the health of the communities we serve.
The Longview project grew out of a Kaiser Permanente adult cooking class recommended for oncology patients, one that focuses on a plant-based diet. Peyer says that after moving to Longview, she and her husband were struck by the limited resources available to the children in the community.
“We wanted to affect change as directly as possible,” says Peyer, an OFNHP/ONA member. “So we dove headfirst into Edible Olympic. We didn’t want to spend time in meetings, we just wanted to get in the dirt and the kitchen—and that’s what we did.”
She sought support from Thriving Schools, one of Kaiser Permanente’s Community Benefit programs. She forged partnerships with the school’s Parent-Teacher Organization and the Lower Columbia School Gardens, a nonprofit that helps schools create garden programs. Local stores donated money. High school students from Longview and Portland also are participating.
“The kids, their parents and the greater community have embraced the efforts and confirmed that our hunches were right,” Peyer says. “Good, healthy, real food, prepared simply, with love and in community, can be life transforming.”
Members of the Oncology unit-based team are supporting the project, too, donating money and time; four KP employees help staff the cooking class.
“Volunteering in the community gives us at KP a chance to share our skills and our approach to supporting good health,” says Elizabeth Engberg, the Northwest’s Thriving Schools program manager. “It also helps us learn about our members—where they live, work, learn and play, because that’s a huge part of what affects their health. Schools are the best place to do this.”
The program has had overwhelming and unexpected participation.
“The idea was that this project would launch with eight to 10 kids. We had 60 kids come to the information session,” Peyer says, which prompted an instant expansion from one to two sessions. The kids work in the garden on Thursday afternoons, and on Fridays, they walk across the field to the middle school, where they are able to use the home economics classroom for cooking class. The sessions run for five weeks and end with a celebration where the kids cook a complete meal and share with their friends and family.
The first session got under way last spring. A grassy patch of the school’s property was selected as the site for the garden, and the children got seeds started indoors. As weather allowed, the ground was prepared. While they waited for their seedlings to be ready to plant, the kids were introduced to kitchen safety and how to prepare the food they were just beginning to grow.
In the cooking class, kids have a healthy snack, then work in small groups to prepare the dish of the week. When the cooking is done, they gather together and enjoy their meal. The kids leave with a bag of groceries so they can cook the meal at home.
“In some cases, this may be the healthiest meal the family may eat during the week,” Peyer says.
On that fall day out in the garden, the kids in the second session organized quickly after studying the garden map Bixby brought along for reference. They divided themselves into groups and got to work with shovels, buckets and plants to complete the day’s activities.
One of the choices they faced was whether to extend the blueberries to the fence or stop a few feet in to allow for a foot path. Several kids piped up with ideas. The decision got made after 11-year-old Christian Aguibar offered his opinion.
“We can grow more things if we don’t have a walkway,” Christian said, “so let’s not have one.”
The Colorado region is improving patient care and saving millions by providing high-risk patients extra attention after discharge, leading to a reduction in readmission rates. In the Post Acute Care Transitions (PACT) program, nurse practitioners visit patients in their homes after discharge from a hospital or skilled nursing facility, giving them a chance to alter the patient’s care plan if needed. The PACT team has visited approximately 4,200 high-risk patients since the program began in January 2013. At that time, 22 percent of high-risk patients were readmitted within 30 days, at a cost of $11.7 million. The PACT team has reduced readmission rates by 50 percent, saving Kaiser Permanente approximately $6 million since the program began.
To make sure no good deed goes uncopied, the Georgia region launched a Spread and Sustain system to move best practices throughout the region—and showed off the results to KP’s board of directors at a UBT fair early last summer. Georgia took a spread blueprint from the Southern California region and fine-tuned it to meet its needs. Now its unit-based teams, sponsors and regional leaders identify projects with good spread potential, determine other locations where the new process could work, share the practice and check back to see how they’re being sustained. Several projects have been successfully spread region-wide—addressing such issues as hypertension, HPV vaccinations and lab specimen collection.
Hawaii is a beautiful place to live, but Kaiser Permanente members who live on the less-populated islands sometimes find it challenging to get the care they need. To address that, KP offers a special benefit called Travel Concierge Service. If health plan members need medical care that isn’t available on their island, KP assists them in traveling to the Moanalua Medical Center in Oahu or to a specialty care medical office. KP makes the travel arrangements and picks up the tab for travel, including airfare, shuttle service and discounted hotel rates. For minors who need specialty care, KP also pays for companion travel. “Our members love this service,” says Lori Nanone, a sales and account manager in the region.
For several years, co-leads in the Mid-Atlantic States have compiled monthly reports of their UBT activities, goals and progress using Microsoft Word and Excel. Now, the region is rolling out a dashboard that automatically compiles the same information from UBT Tracker into an easy-to-reference SharePoint site, Kaiser Permanente’s new online social collaboration tool. The new dashboard will encourage more frequent updates to UBT Tracker and eliminate the need for co-leads to create separate documents, says Jennifer Walker, lead UBT consultant and improvement advisor. “Now the information we get is more timely and easier to assess,” Walker says. “Before, the information was up to a month old.”
The Santa Rosa Medical Center Diversity Design committee is equipping employees with tools to help them provide better service to Spanish-speaking patients. The group, composed of labor and management, has been piloting a handout featuring a list of common Spanish phrases, such as ¿Necesita un intérprete? (“Do you need an interpreter?”), as well as instructions on using the phone interpreter system. The idea came from a Spanish-speaking patient on the facility’s Latino patient advisory committee, who recalled the time she was lost in the facility and no one could direct her in Spanish. The Spanish language flier is the latest in the committee’s work to help ensure all patients receive the same optimal service and care.
Unit-based teams in the Continuing Care Services department are focusing on improving the experience for some of Kaiser Permanente’s most vulnerable members: those in skilled nursing facilities or receiving home health, hospice or palliative care. Teams are focusing on ensuring better transitions for patients as they go from inpatient to ambulatory care. By identifying issues before they become problems, labor and management hope to coordinate care more effectively, reduce emergency department visits and cut down on outside medical costs.
Harmony comes easily when you use the tools of partnership. Just ask the Biohazards, a band of union members and a manager that uses partnership principles to guide performances. “We call ourselves an LMP project,” says Mary Anne Umekubo, a clinical laboratory scientist and Regional Laboratory assistant director who sings and plays percussion and guitar. She is among six band members who represent a variety of departments, shifts and unions, including SEIU-UHW and UFCW Local 770. Performing for friends and colleagues, band members use consensus decision making to choose songs, interest-based problem solving to fix mistakes and the Rapid Improvement Model to tweak performances. “We’re from different departments,” says drummer Eric Cuarez, a regional courier driver and SEIU-UHW member. “We come together to play music.”
Like casts and splints, X-rays are a routine part of patient care in the Orthopedics department at South Bay Medical Center. Unfortunately, missed copays for those X-rays were becoming common as well.
“Patients will get their X-rays done at the end of the visit—and then walk out without realizing that they owe a copay,” says Christopher Kresch, department administrator for Orthopedics and the team’s management co-sponsor. At other times, patients will unexpectedly need X-rays during their visit, and because the orders are placed during the exam, the charges are not captured during check-in.
So the team borrowed a practice from the Los Angeles Medical Center and developed a check-in sheet that shows, at a glance, if a patient has an outstanding X-ray copay. The team also adjusted its workflow to ensure that a staff member walks the patient to the front desk to pay the fee by the end of the visit.
Here’s how the process works:
The receptionist gives the check-in sheet to each patient at the start of the visit. As patients travel through the clinic to receive care, the form goes with them, enabling staff to conduct “warm hand-offs” by writing notes to each other about the patient’s care. When a copay is owed, the last person to interact with the patient escorts him or her to the receptionist.
“It helped us in a lot of different ways, much more than we thought it would,” says Naomi Guerrero, an Orthopedic technician and SEIU-UHW member who is the team’s union co-lead. “Now we can’t live without it.”
After introducing the check-in sheet, the team saw almost immediate improvement in copay collection. In July 2014, missing copays—known as the total collected variance—totaled $2,166. Between August and November 2014, the total collected variance fell to just $533, a whopping 75 percent improvement. Those numbers are holding steady. The department is averaging a 50 percent increase in copay collections through third quarter 2015.
Besides boosting copay collection, the check-in sheet helped the team improve patient care. Unexpected benefits include:
Before adopting the check-in sheet, the team sought input from a group of staff members and physicians in the department. Incorporating their voices gave them ownership of the project and enabled the team to create a check-in sheet that worked for everyone. For example, physicians rejected an early draft featuring a detailed checklist in favor of blank space to write their orders. And receptionists vetoed an early color-coding system as “too confusing.”
“We learned a lot as we went through our tests of change,” says Guerrero. “We learned there are changes that don’t work out.”
Once team members were happy with the check-in sheet, they spread it to the rest of the department. Convincing their peers to consistently use the check-in sheet took time.
“The medical assistants were resistant because they saw the check-in sheet as an extra step,” says UBT representative Zackry Ellis, a physician assistant and member of UNAC/UHCP.
Some providers also were hesitant to use the form, preferring to speak with staff. That’s when the team turned to Anthony Leone, MD, the department’s physician chief, for help.
“He helped us sway others to try it out,” Guerrero says.
Once staff members understood the benefits of the check-in sheet—enhanced copay collection, improved workflow and better patient care—they all began to use it consistently.
Patients are reaping the benefits of the new form, too.
“Because of the check-in sheet, we’re communicating more with our members,” says UBT representative Esmeralda Montes, a lead medical assistant and SEIU-UHW member. “They feel happy and cared for, and that’s our ultimate goal.”
Format:
PDF
Size:
1 page, 8.5" x 11"
Intended audience:
Unit-based team members, team co-leads, sponsors and safety leaders
Best used:
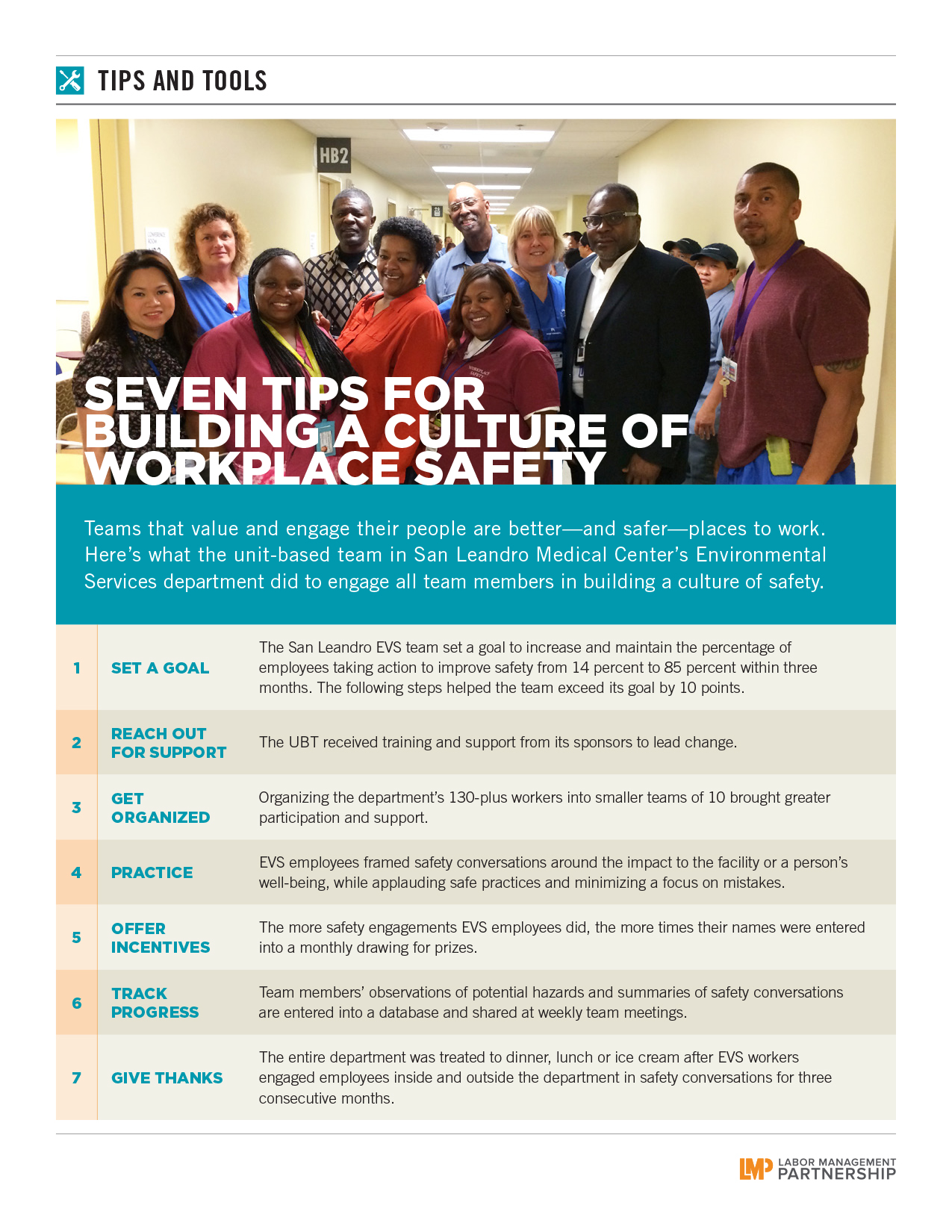
Seven steps that helped one EVS team change the culture and reduce workplace injuries. Use to encourage workplace safety conversations and practices that have worked elsewhere.
For years, success eluded the Baldwin Park Critical Care team. Mired in distrust, staff members didn’t participate in unit-based team meetings. As recently as 2011, few in the 49-member department knew the team existed.
“I didn’t even know what UBT stood for,” says Sheryl Magpali, RN, a member of UNAC/UHCP and now the team’s union co-lead. “No one claimed to be part of it. It was pretty much nonexistent until 2013.”
With a new manager on board, interest in the UBT grew. Staff members from the Critical Care Unit and its sister department, the Step-Down Unit, elected 12 representatives, who in turn chose Magpali as the labor co-lead. Celso Silla, RN, the new department administrator, became the management co-lead.
It was rough going at first.
Attendance was spotty. When the team did meet, members focused on long-simmering grievances about labor and personnel issues. The team reached out to Charisse Lewis, Baldwin Park’s UBT consultant. While consultants often focus on helping teams with using the Rapid Improvement Model and designing tests of change, they also help teams learn to work as teams—clearing up issues that are distracting them from the work at hand.
Lewis’s first steps were to encourage the team’s union members to meet separately with a labor representative.
“That helped relieve the stressors of the union issues,” Magpali says. Now, she says, “team meetings focus on changes that affect the unit, rather than things we have no control over.”
The department—nearly all nurses, but also including ward clerks, who are SEIU-UHW members and one of whom is a team representative—began building trust in other ways, too. At Lewis’s suggestion, staff members organized a bowling night and had dinner together. This summer, they held a backpack drive.
“Charisse has been good at guiding us—attending our meetings, observing and listening and seeing how we can do better,” says Silla.
Lewis didn’t stop with team-building activities. She coached Magpali, a soft-spoken nurse, to speak up during meetings and make her voice heard, and she helped Silla overcome his reluctance to leave his union co-lead in charge of meetings.
Once trust was established, the team could turn its attention to improving patient care, with remarkable results. UBT members have reduced central line-associated bloodstream infections from five in 2014 to none as of August of this year. Buoyed by that success, they are working to reduce catheter-associated infections.
Silla attributes the improvements to the culture of partnership and putting frontline employees in charge of decisions that affect their work.
“We would have been in limbo” without Lewis’s guidance, Silla says. “Now we’re on the same page. We can be a Level 5 in the future.”