Staff Directory
Full Directory
Kizmet Knox
Phone:
(470) 714-1637
Email:
Kizmet.Knox [at] kp.org
This short animated video explains how to find and use our powerful how-to guides
Does your team want to improve service? Or clinical quality? If you don't know where to start, check out the team-tested practices on the LMP website. This short video shows you how.
Having trouble using the search function? Check out this short video to help you search like a pro!
Need to find a checklist, template or puzzle? Don't know where to start? Check out this short video to find the tools you need on the LMP website with just a few clicks.
The Colorado region is improving patient care and saving millions by providing high-risk patients extra attention after discharge, leading to a reduction in readmission rates. In the Post Acute Care Transitions (PACT) program, nurse practitioners visit patients in their homes after discharge from a hospital or skilled nursing facility, giving them a chance to alter the patient’s care plan if needed. The PACT team has visited approximately 4,200 high-risk patients since the program began in January 2013. At that time, 22 percent of high-risk patients were readmitted within 30 days, at a cost of $11.7 million. The PACT team has reduced readmission rates by 50 percent, saving Kaiser Permanente approximately $6 million since the program began.
To make sure no good deed goes uncopied, the Georgia region launched a Spread and Sustain system to move best practices throughout the region—and showed off the results to KP’s board of directors at a UBT fair early last summer. Georgia took a spread blueprint from the Southern California region and fine-tuned it to meet its needs. Now its unit-based teams, sponsors and regional leaders identify projects with good spread potential, determine other locations where the new process could work, share the practice and check back to see how they’re being sustained. Several projects have been successfully spread region-wide—addressing such issues as hypertension, HPV vaccinations and lab specimen collection.
Hawaii is a beautiful place to live, but Kaiser Permanente members who live on the less-populated islands sometimes find it challenging to get the care they need. To address that, KP offers a special benefit called Travel Concierge Service. If health plan members need medical care that isn’t available on their island, KP assists them in traveling to the Moanalua Medical Center in Oahu or to a specialty care medical office. KP makes the travel arrangements and picks up the tab for travel, including airfare, shuttle service and discounted hotel rates. For minors who need specialty care, KP also pays for companion travel. “Our members love this service,” says Lori Nanone, a sales and account manager in the region.
For several years, co-leads in the Mid-Atlantic States have compiled monthly reports of their UBT activities, goals and progress using Microsoft Word and Excel. Now, the region is rolling out a dashboard that automatically compiles the same information from UBT Tracker into an easy-to-reference SharePoint site, Kaiser Permanente’s new online social collaboration tool. The new dashboard will encourage more frequent updates to UBT Tracker and eliminate the need for co-leads to create separate documents, says Jennifer Walker, lead UBT consultant and improvement advisor. “Now the information we get is more timely and easier to assess,” Walker says. “Before, the information was up to a month old.”
The Santa Rosa Medical Center Diversity Design committee is equipping employees with tools to help them provide better service to Spanish-speaking patients. The group, composed of labor and management, has been piloting a handout featuring a list of common Spanish phrases, such as ¿Necesita un intérprete? (“Do you need an interpreter?”), as well as instructions on using the phone interpreter system. The idea came from a Spanish-speaking patient on the facility’s Latino patient advisory committee, who recalled the time she was lost in the facility and no one could direct her in Spanish. The Spanish language flier is the latest in the committee’s work to help ensure all patients receive the same optimal service and care.
Unit-based teams in the Continuing Care Services department are focusing on improving the experience for some of Kaiser Permanente’s most vulnerable members: those in skilled nursing facilities or receiving home health, hospice or palliative care. Teams are focusing on ensuring better transitions for patients as they go from inpatient to ambulatory care. By identifying issues before they become problems, labor and management hope to coordinate care more effectively, reduce emergency department visits and cut down on outside medical costs.
Harmony comes easily when you use the tools of partnership. Just ask the Biohazards, a band of union members and a manager that uses partnership principles to guide performances. “We call ourselves an LMP project,” says Mary Anne Umekubo, a clinical laboratory scientist and Regional Laboratory assistant director who sings and plays percussion and guitar. She is among six band members who represent a variety of departments, shifts and unions, including SEIU-UHW and UFCW Local 770. Performing for friends and colleagues, band members use consensus decision making to choose songs, interest-based problem solving to fix mistakes and the Rapid Improvement Model to tweak performances. “We’re from different departments,” says drummer Eric Cuarez, a regional courier driver and SEIU-UHW member. “We come together to play music.”
Unit-based teams are hitting their stride, with 190 out of 261 teams reaching a Level 4 or 5 on the five-point Path to Performance. Teams are engaged in several types of projects, including those that save the organization money. The region will see a financial savings of $1.85 million this year through the 175 affordability projects of UBTs. The five UBT consultants in the region are coaching teams impacted by regional restructuring and helping those teams rebound quickly. Teams also are focusing on workplace safety, patient safety and HEDIS measures (Healthcare Effectiveness Data and Information Set).
Starting in May and running through December 2015, Georgia medical centers are conducting an experiment. This region-wide test involves using greeters to usher in members. During the trial period, 15 greeters will make the member feel welcomed and convey the message they are important to Kaiser Permanente. Greeters also will answer questions, escort members to their appointments, maintain waiting rooms, ensure wheelchairs are available and welcome members with a smile. “They will provide a concierge-type member experience,” says Elizabeth Ramsey, the Georgia region’s senior manager of loyalty and retention.
The Hawaii region recently re-set its 57 unit-based teams’ scores on the Path to Performance to Level 1. Three consultants—two also are registered nurses and one is a project manager—will help teams quickly advance as they meet such core requirements as sponsor training. The region is unique in that, for now, one union (Hawaii Nurses Association/OPEIU Local 50) is in the Coalition of Kaiser Permanente Unions, while other unions are not. Although that can be challenging, consultants say teams still focus on the patient and want to do improvement work. “We help each other work through obstacles with our teams and understand the data,” says Lisa Kane, UBT consultant and project manager.
In February, when home health orders came in to Health Information Management Services Northern Virginia, the average turnaround time was 4.4 days. By creating red folders for the orders, adding a cover sheet that says “stat” and date stamping the order as soon as it arrives, the team cut turnaround time to three days by April 2015—even as the number of orders went up from 673 in February to 747 in April. “This was important to the workflow, because when home health agencies called to follow up on the orders it interrupted our work,” says LaShawnda Powell, a senior health information management assistant in Woodbridge, Virginia, and member of OPEIU Local 2. “We have determined that our new process is successful and we’ve adopted it.”
Last year, unit-based team consultants and union partnership representatives formed a regional UBT to work on issues related to consistency and accountability for Northern California’s 1,300 frontline teams. Now the group has established three subgroups to review the 2015 National Agreement, which includes new provisions for UBTs. Each subgroup has a distinct focus area: sponsorship, UBT validation and assessment, and tools to support contract expectations. The subgroups will develop recommendations for review by a committee of labor members and management representatives. The regional co-leads will submit final recommendations to the regional LMP Leadership Council by year’s end.
UBT Resource Team members have been busy refining the region’s new process for assessing teams on the Path to Performance. Co-leads and sponsors of 415 unit-based teams in the Northwest work with their consultant to ensure each team advances or sustains high performance throughout the year. Improvement Advisors help co-leads create action plans and provide direct training to move teams along or refer them to the appropriate subject matter experts. A majority of teams at Levels 2 and 3 will advance to high performance within the next 90 days due in large part to the work of the UBT Resource Team.
Playing games at work usually is considered taboo. But that’s exactly how a group of regional UBT staff members spent a recent afternoon when they learned to play the “Leading Innovation Game.” Created by Kaiser Permanente’s Innovation and Advanced Technology team, the board game is designed to help employees overcome challenges that can doom the best ideas. Starting this fall, regional UBT staff will train team co-leads and sponsors, who will share the game with unit-based teams at their facilities. “Most teams come up with great ideas but they aren’t always aware of potential pitfalls,” says Rosalyn Evans, UBT practice leader for Southern California. “This board game gives them hands-on experience to develop innovation in a risk-free environment.”
Patient safety is about more than the hands-on care delivered in a hospital or clinic. It’s also about what caregivers do to close care gaps and be sure patients get the care they need.
To ensure this happens with every abnormal prostate, breast, pelvic, osteoporosis and fecal exam, the Georgia region established a centralized Outpatient Safety Net Program. Almost four years ago, borrowing techniques from Southern California’s successful safety net program, the Georgia region dedicated the equivalent of four full-time and one part-time nurse. Their jobs: to continue reaching out to patients who don’t respond to an initial contact regarding an abnormal test result.
The program is saving lives—and has earned KP’s 2014 David M. Lawrence Patient Safety Award in the transfer category, an award for a region that successfully implements a project from an earlier award winner. The Southern California safety net system had won a 2012 Lawrence award for its work.
“If you have an abnormal stool test, you should be seen in gastroenterology,” says Rahul Nayak, MD, who served as physician program director of patient safety for Georgia when the program launched. “It will raise a red flag in our system if that doesn’t happen in a certain amount of time. That’s why it’s called a safety net—it’s the net below the tightrope walker.”
Sonja “Patrice” Evans, RN, is the manager of Georgia’s outreach effort and leads the group of nurses. She also steps in to convince members who initially say they don’t want to come in for further testing. “We can prevent something small from turning into something big,” she says.
The nurses receive a list of patients who have abnormal results. They make two attempts to reach them by phone and send a certified letter if the calls don’t work. “Our team tries to catch a small group of patients before they fall through the cracks,” Evans says.
So far, it’s working.
In 2013, the most recent year for which data are available, 4,000 members were contacted about abnormal breast exam results. Of those, 93 percent were successfully scheduled for a follow-up appointment within the prescribed seven days. For abnormal pelvic exam results, 2,000 members were contacted, and 95 percent of those were scheduled within seven days.
Five hundred members—most of whom had declined or not responded to previous contacts—were reached within 100 days of abnormal prostate exam results; 87 percent scheduled a follow up. The team contacted 200 members with abnormal osteoporosis exam results, and more than 70 percent scheduled a follow up within 30 days, which exceeded the Medicare 5-Star guidelines.
Dr. Nayak, UBT co-lead for gastroenterology at Southwood Medical Center, says one of his patients benefited from the program.
“Our safety net caught a positive (fecal occult blood test) that I had missed two months prior,” he said when accepting the Lawrence award on behalf of the team. “That patient had an advanced adenoma which was well on its way to malignancy. Without the safety net, there is no guarantee that we would have found this polyp” in time.
Now, Georgia’s program is expanding and will include other types of patient notifications.
Format:
PDF
Size:
8.5” x 11”
Intended audience:
Frontline employees, managers and physicians
Best used:
This postcard features a GI team and how it cut costs by hiring fewer contract physicians and refining scheduling of staff and patients. Post and use it to spur discussion in UBT meetings.
Sometimes the best way to spread effective practices is to spread experienced people. That’s what happened when the Alpharetta Ob-Gyn UBT in Georgia zoomed from Level 1 to Level 4 in just 10 months after two nurses from two different high-performing UBTs transferred there at the same time.
Jane Baxter and Ingrid Baillie had been UBT co-leads at two different clinics when they each got a new job with the Alpharetta Ob-Gyn department. They both drew on their experiences to guide their new team when they became co-leads at Alpharetta. “We knew the steps in the process and what to expect,” says Baxter, the department’s charge nurse.
Fledgling teams should begin with small performance improvement projects, they say. “We started with the low-hanging fruit,” says Baillie, RN, a member of UFCW Local 1996. “You don’t need to reach for the stars right out of the box.”
And, says Baillie, there’s no need to look any further than Kaiser Permanente’s organization-wide and regional priorities to find plenty of ideas for performance improvement projects—and a wealth of data that is being collected regularly.
“KP makes no secret about what is important to it,” says Baillie. “From that alone, you have all the data you need.”
For instance, the Alpharetta team’s first efforts were to improve clinic start time and get a second blood pressure test for patients with high initial readings. “These are important to KP, and they helped us gel as a team,” says Baillie.
“Small wins help develop confidence,” says Baxter. Now the team is taking on more complex cross-departmental initiatives, such as trying to make available online the big packet of paperwork patients need to complete before a first Ob-Gyn visit.
Getting physicians involved also has been part of this UBT’s success. You won’t find doctors who think UBTs are just for clinic staff on this team, says Baxter.
“Our providers are very invested,” she says. “They take minutes at meetings. We are all on an equal playing field.”
On one level, the pediatric clinic at Georgia’s Panola Medical Center Offices is like any other pediatric clinic. Babies squawking and squealing are part of the soundtrack—and under that, there’s the murmur of parents and nurses cooing to get the little ones to stop crying.
But the Panola clinic’s unit-based team stands out. Its members work at one of the several pediatric clinics in KP’s Georgia region that have significantly improved preventive care and screenings for their young patients, who range in age from newborn up through their teens.
The pediatric teams have achieved these goals in the midst of competing demands by staying laser-focused on a handful of quality measures in the Healthcare Effectiveness Data and Information Set, or HEDIS.
“Our projects are usually HEDIS-related,” says Panola’s labor co-lead, Sheryl Boyd, a licensed practical nurse and member of UFCW Local 1996. “HEDIS is so measurable.”
The work is a good example of how, instead of driving an agenda from the top down, achieving a goal can be inspired by engaging frontline teams in understanding how they contribute to KP’s brand promise of total health.
“The teams are not ‘being told what to do,’ but rather they see the big picture and see what they can do to affect it,” says David Jones, MD, Georgia’s physician co-lead for UBTs. Dr. Jones says he and his labor and management LMP counterparts stay abreast of Georgia’s regional goals and priorities, then work with UBT consultants to communicate those to frontline teams.
“We incorporate UBTs as a lever to execute our clinical goals,” says Dr. Jones, creating a vital loop of communication and support.
One of the Panola UBT’s successes has been to increase the number of girls getting the human papillomavirus vaccine (HPV) by their 13th birthday. The vaccine can help prevent a virus that increases the risk of cervical cancer.
The project kicked off in October 2011. At the time, the team wasn’t tracking how many of the girls in the target population had received the vaccination, which is delivered in a series of three shots over six months. The team’s initial goal was to get 5 percent of the girls eligible for the shot vaccinated. In the first six months, the team succeeded in getting 10 percent of the target population started on the series—and by October 2013, nearly 20 percent had gotten the complete series, a significant achievement. While it has yet to reach the national HEDIS average for the vaccination, the team is steadily closing the gap.
Team members achieved these results by working with the clinic’s information technology staff to get a list of patients—11- and 12-year old girls—who needed the vaccine. They contacted parents and made appointments. In the exam room, nurses discussed HPV and the importance of the vaccine with patients and their parents.
And they worked with their IT colleagues again, modifying the computer system so they could book appointments six months in advance. That allowed them to act on a crucial step—scheduling visits for the two follow-up booster shots right then and there.
The parent education was extremely important, says Erica Reynolds, the charge nurse and management co-lead.
“Some parents think we want people to come back in for appointments because we want the co-payments,” she says—but in fact, if the shots aren’t completed in the proper time period and the immunization series needs to be started all over, it requires even more visits. To avoid that, she says, “Scheduling a nurse visit for the second and third vaccines has become a part of our workflow.”
That kind of hard-wiring of successful practices is the holy grail of performance improvement.
As labor co-lead Boyd puts it, “Our projects are not ‘projects.’ They are ongoing.”
In addition, Dr. Jones says, the integration of partnership and performance is taking place at all levels in the region.
For example, he says, physician leaders “integrate the Labor Management Partnership and performance improvement into existing meetings so it is not viewed as outside those discussions.”
As a result, when Georgia earned a five-star Medicare rating in fall 2013 for the first time—bringing all of KP’s regions into that rarified club of health care excellence—Rob Schreiner, MD, the region’s executive medical director, specifically credited UBTs and the culture of continuous improvement for the achievement.
Driven by those two engines, says Schreiner, “We’ll improve quality, service and affordability at a tempo that exceeds that of our competitors.”
Louise Dempsey is the business representative for UFCW Local 1996 in Atlanta. She spoke with LMP communications consultant Laureen Lazarovici about her experiences as a union activist in the South.
In the late ’60s and early ’70s, my mom worked for the Social Security Administration. She transferred often for her job, so we moved a lot. She was in the union, and she organized two of the offices she got transferred to in order to get better benefits. One was in the hills of Tennessee, where there were a lot of coal mines and a lot of poverty. She once worked for a group of attorneys and mobilized her co-workers to get better wages. There was a lot of disparity in pay in terms of gender and race. Sometimes, they didn’t exactly like her. She earned the reputation as the go-to person. People would say, “If anybody can get it done, it’s Mildred.”
And today, here we are in the South. It is not strong union territory. Because of Georgia’s so-called “right to work” law, employees can work for KP here whether they join the union or not [in contrast to KP regions in other states with stronger worker protection laws]. But people join because they know that the stronger we are, the more we can stand up for ourselves. We have to talk to folks about the benefits of working for a unionized company. I worked for KP as an LVN before there was a union. Our wages were all over the place and assignments were based on favoritism. We’ve had people come to work for KP because it’s unionized.
When they hear about the Labor Management Partnership, they say, “I’ll sign up.” They understand they have a voice, they can be part of a UBT, they can affect the direction their team is going, and say what they need and want and be heard. Sure, we have to educate managers, but we have to educate employees about unions, too. When I talk at new employee orientation, I tell them we are there as a mediator, facilitator, advisor. You are not by yourself anymore. I’ve got your back and your front and your side, too. With the Labor Management Partnership, KP is always offering opportunities for employees to learn, like the Ben Hudnall Memorial Trust. I have been in the medical field for 30 years, and folks are always thirsting for more knowledge.
Folks in management come into Kaiser and they are not used to unions or the partnership. We have to educate them: We have a union, we have a contract, we have a partnership. We educate them about a union environment and also that we are not the traditional head-butting adversarial union.
Normally, when I go into a meeting at KP, there is not a whole bunch of posturing. People want to get to a solution. There is no name-calling, finger-pointing or yelling. It makes a difference. Partnership benefits the local because I have open access to the employees. I went to five facilities recently. I was not stopped once. It is always, “Hi, how are you, who do you need to see?” My co-workers at the local who represent employees at other companies don’t all have that. KP has not relegated me to a break room or to certain hours. I can have a bulletin board in the break room. I have the time to speak with new hires during orientation. They don’t censor the questions the employees ask or the ones I answer. That’s partnership.
Format:
Powerpoint
Size:
41 pages
Intended audience:
Frontline employees and managers
Best used:
These slides were presented by three teams that shared their outstanding work on patient safety in a virtual UBT Fair in March, 2013. Use to spread best practices on patient safety.
The teams featured are:
Format:
PDF
Size:
8.5” x 11”
Intended audience:
Frontline employees, managers and physicians
Best used:
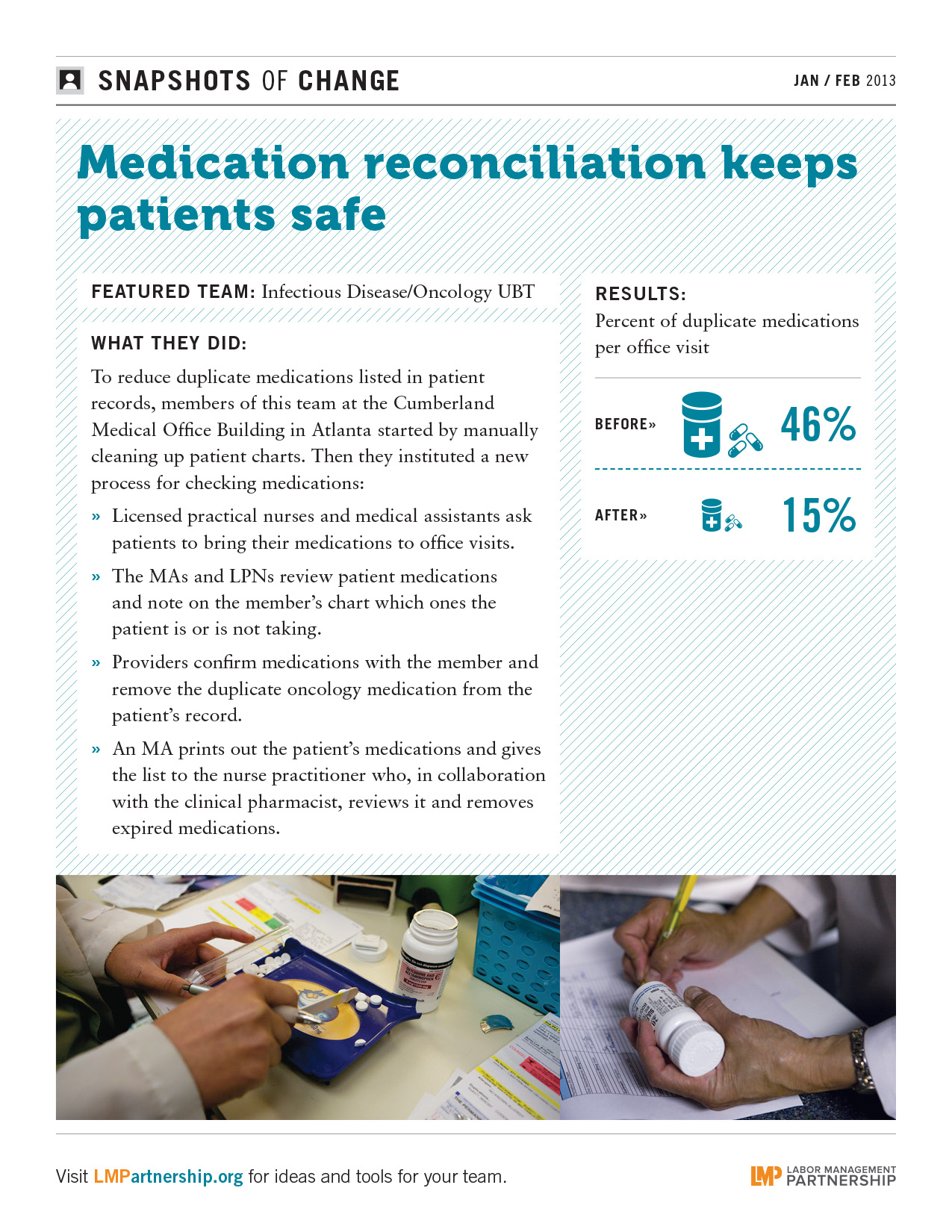
This poster highlights a Georgia team that reduced duplicate medications listed in patient records. Post on bulletin boards, in break rooms and other staff areas.