TOOLS
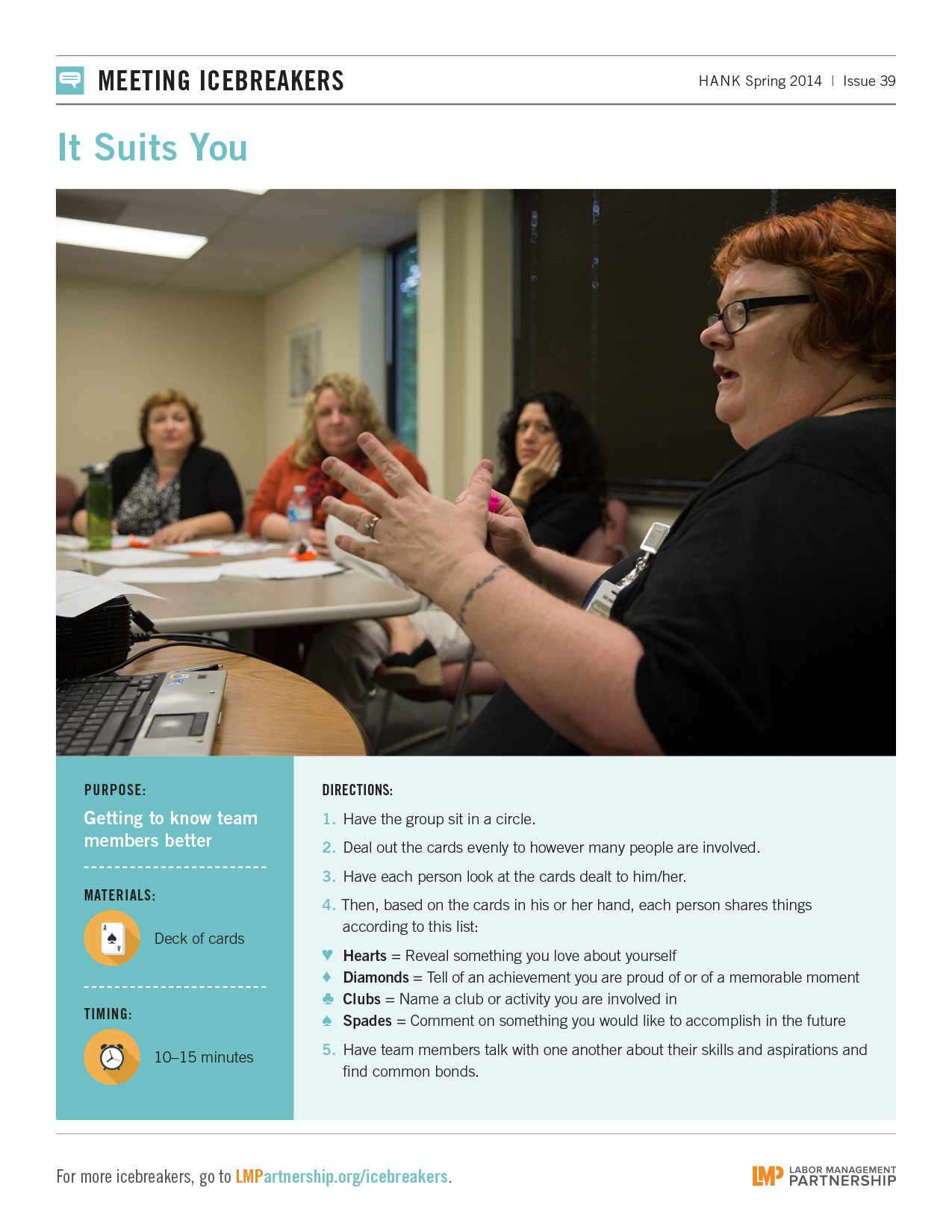
Icebreaker: It Suits You
Format:
PDF
Size:
8.5” x 11”
Intended audience:
Frontline employees, managers and physicians
Best used:
Use this meeting icebreaker to get to know your team members better. From the Spring 2014 Hank.
This short animated video explains how to find and use our powerful how-to guides
Does your team want to improve service? Or clinical quality? If you don't know where to start, check out the team-tested practices on the LMP website. This short video shows you how.
Having trouble using the search function? Check out this short video to help you search like a pro!
Need to find a checklist, template or puzzle? Don't know where to start? Check out this short video to find the tools you need on the LMP website with just a few clicks.
Format:
PDF
Size:
8.5” x 11”
Intended audience:
Frontline employees, managers and physicians
Best used:
Use this meeting icebreaker to get to know your team members better. From the Spring 2014 Hank.
Format:
PDF
Size:
8.5” x 11”
Intended audience:
Frontline employees, managers and physicians
Best used:
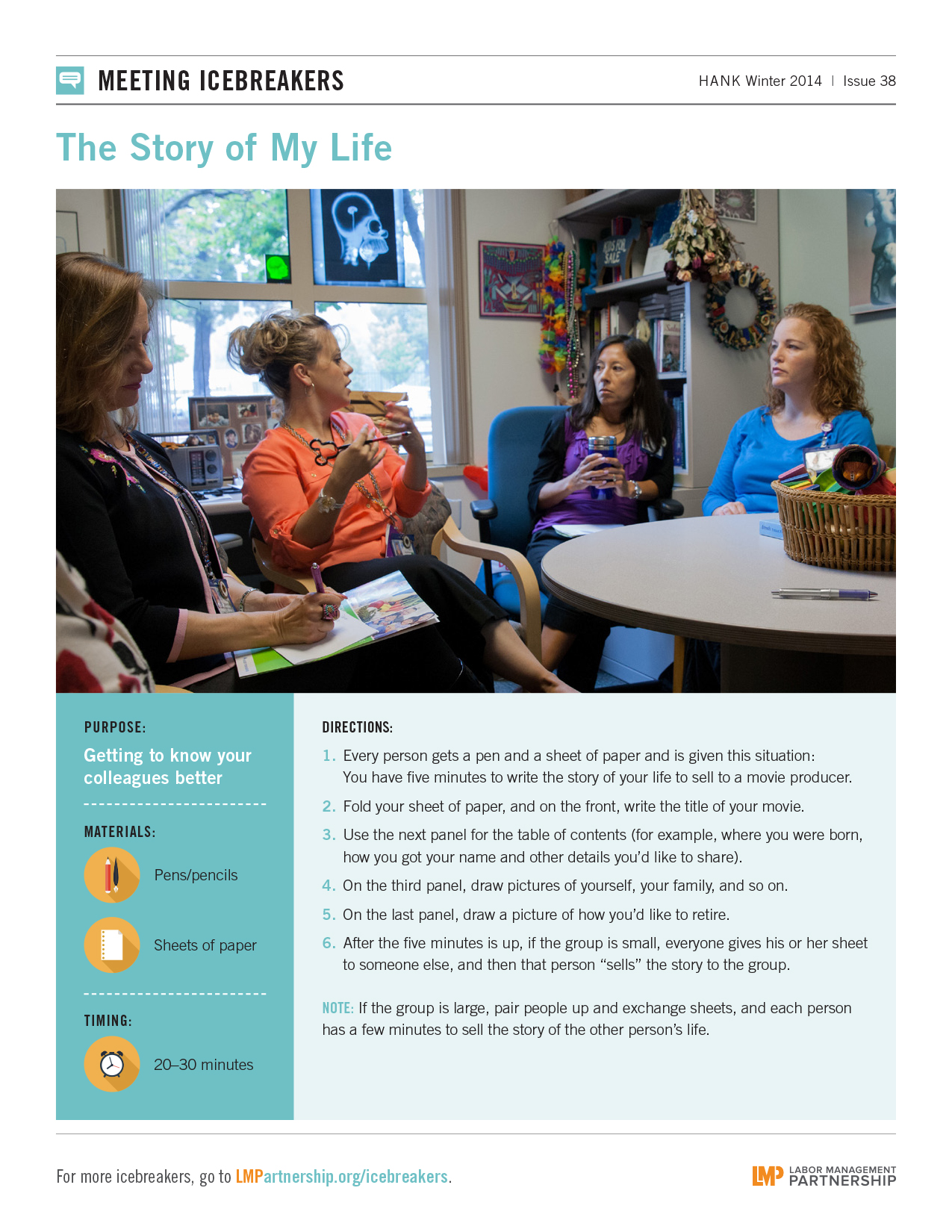
Use this meeting icebreaker to get to know your colleagues better.
Format:
PDF
Size:
8.5” x 11”
Intended audience:
Frontline employees, managers and physicians
Best used:
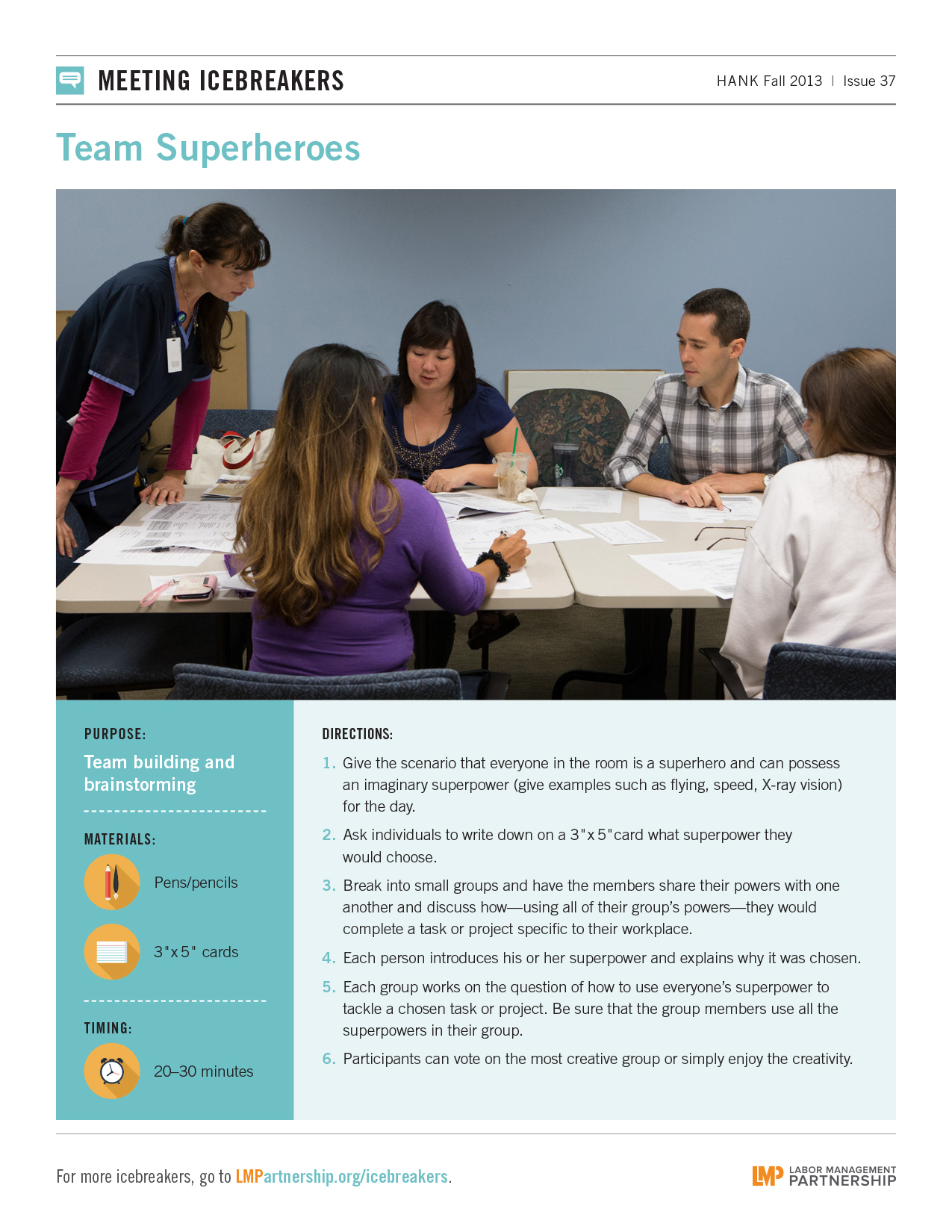
Use this meeting icebreaker to do team building and brainstorming. From the Fall 2013 Hank.
Format:
PDF
Size:
8.5” x 11”
Intended audience:
Frontline employees, managers and physicians
Best used:
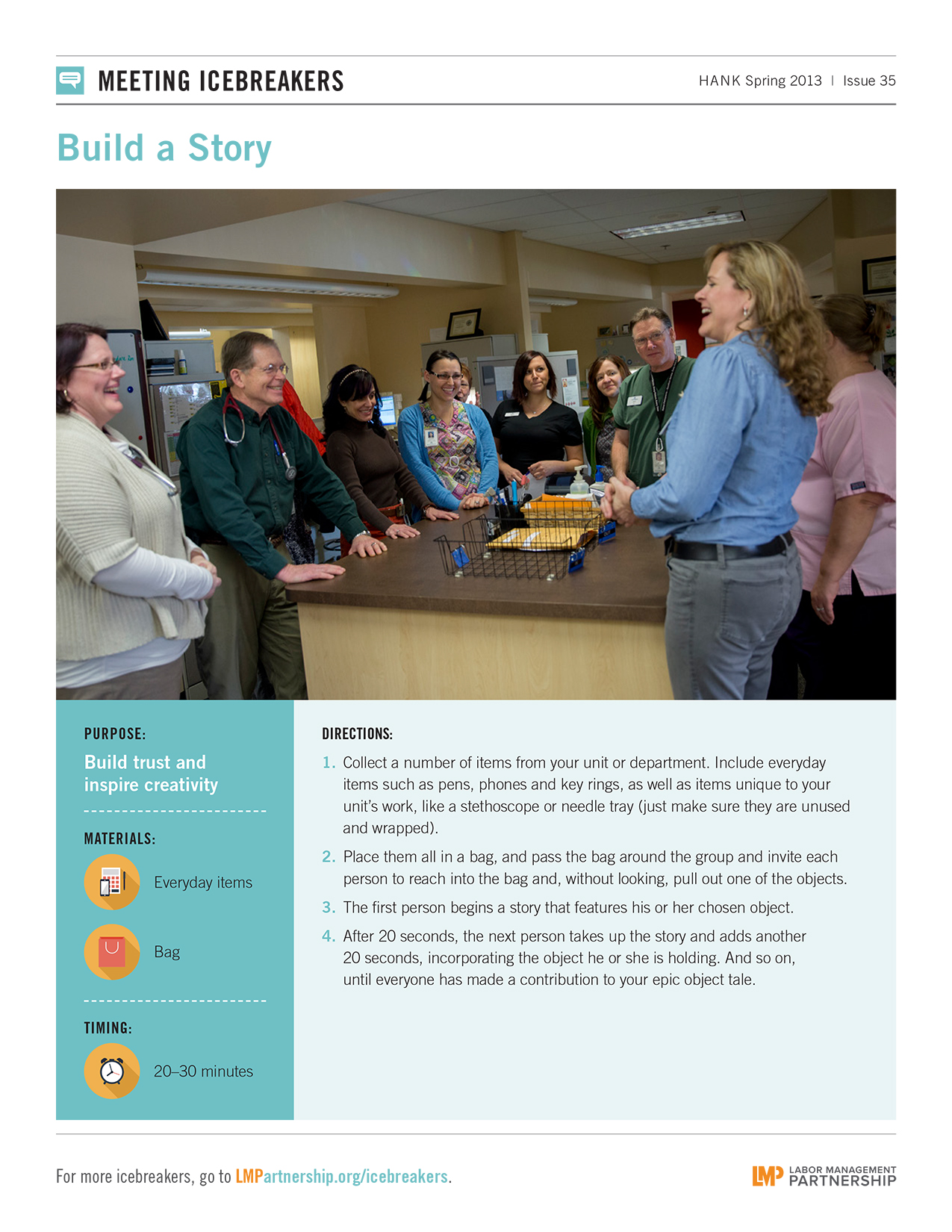
Use this meeting icebreaker to build trust and inspire creativity with team members.
Format:
PDF
Size:
8.5” x 11”
Intended audience:
Frontline employees, managers and physicians
Best used:
Use this meeting icebreaker to find out interesting things about your team members.
Bernie Nadel is director of customer service and call center operations at Patient Financial Services in Southern California. He co-chairs the Regional Operations LMP Council, bringing together 27 business units, including the regional laboratory, central refill pharmacy and optical services.
None of us was born into a unit-based team. Partnership is learned. Teams and their leaders need guidance and a playbook.
I tell other managers partnership makes my job easier. I have 10 other people helping to come up with solutions. I know some managers are uncomfortable with that approach. They act as though they can opt out of the Labor Management Partnership. It’s as if they said, “I know we have KP HealthConnect™, but I want to use this other computer program.” I say, if you don’t want the LMP, don’t work at Kaiser Permanente. You don’t get to opt out of the company’s policy.
Recently, our UBT went through a list of issues to work on. Call volume is up 30 percent, and we’re figuring out how to deal with that. We are going to do several tests of change. UBT members are gung ho about it. If I were to try to make those changes myself, I’d miss things. I would not get the insights of the people who interact with our members every day. And the people doing the work wouldn’t have the ownership and energy that comes with having a voice. Employees know I believe in partnership—and I give them the time to do it. That is a challenge. But you can’t solve the problems if you don’t invest.
Not that long ago this call center was a toxic environment. There was low trust and low morale. All that has switched 180 degrees. A big step was my predecessor attending a sponsorship training class, which led her to involving UBTs more in day-to-day operations. I wanted to build on that.
LMP is a dance between labor and management, and management has to take the first step. When labor sees that management is serious, that’s when it changes. We’ve shown that you can change the culture.
Recently, we had a meeting with top executives about improving the consumer financial experience. Our UBT representative group prepared a report, and it gave our executives insights they couldn’t get any other way. It was not slick, it was real. I’m grateful to the group for the experience, commitment and knowledge they bring to this work every day.
On her last day at work before going on maternity leave, something started going wrong with Juanita Ichinose’s pregnancy—and she found herself in an ambulance, on her way to the Downey Medical Center. Her husband, Trav, followed in his car. The images from an ultrasound foretold a grim story: Juanita was expecting twins, but one of the boys was not moving. “Code Pink” began blaring from the overhead speakers as she was wheeled to the operating room. What caregivers and the family feared came to pass. One twin survived, but the other did not.
“We had some moments with our other son,” says Trav Ichinose. “Then I went to see Teo. He weighed a pound and a half. The doctor told me, ‘He is very small.’”
Thus began Teo Ichinose’s four-month stay in the neonatal intensive care unit, a journey that led his father to become an active member of the department’s parent advisory council. Today, Teo is a happy 4-year-old, obsessed with his toy airplane from the latest Disney movie. And his father continues to bring the voice of the patient to Downey’s NICU unit-based team, where his input has helped shape numerous improvements.
UBTs exist to include all voices—employees, managers and physicians—in efforts to improve performance. And some UBTs are bringing in one more crucial voice: the patient’s.
To be sure, there are UBT members who resist. Objections range from “we don’t have time” to “patients can’t possibly know how our department runs.” But for others, it is a step that literally brings the patient-and-member focus of the Value Compass to life.
“UBTs have a lot of expertise. They know what is and isn’t working,” says Hannah King, director for service quality for unit-based teams. “What is missing is the perspective of the user, someone who might be afraid or in pain. We don’t know what they go through before and after they come to us. So we need to ask.”
Read on to see how UBTs have included patients and members in their work and improved performance.
During his son’s four-month stay in the NICU, Trav Ichinose became concerned that parents were prevented from visiting during shift changes, when the Nurse Knowledge Exchange Plus occurs.
“Parents want to maximize their time with their babies, and the policy was undermining that,” he says.
Nurses wanted to integrate parents into the process but also needed to prevent interruptions. “During the report, the parents tended to interject,” says Marnie Morales, RN, the team’s union co-lead and a UNAC/UHCP member. “That was a safety issue,” because it is important nurses not get sidetracked.
So, together with Ichinose and the parent advisory council, UBT members devised a system that met the needs of caregivers and parents. There would be “quiet time,” when parents listen and jot down notes while the outgoing nurse updates the incoming nurse. Once they’re done, it’s the parents’ turn to discuss their baby’s care with the nurses.
In testing the process, the nurses realized they needed to be able to discuss sensitive information out of the parents’ earshot—if, for example, there was a domestic violence situation or mental health problems in the family. So they came up with a discreet cue that signals the need to step away.
“The patient is getting better care because there is better communication. Information that wasn’t getting shared before is now,” Morales says. “As nurses, we get so involved with charting that we forget the patient is sitting there. Now, we are explaining as we are doing it because the parent is there watching.”
The change gave the team a boost in its satisfaction scores, which rose from 74 percent in the third quarter of 2012 to 88 percent one year later. It works to maintain the scores by holding refresher trainings with staff.
“With long stays like ours, your emotional resilience is tested to the max,” Ichinose says. “There are things that happen in the NICU setting that can undermine that resilience—or bolster it. Bolstering our ability to take in information, to be physically and emotionally present for the care of our child, affects our satisfaction with the care.”
Why do patients fall when they are in the hospital? Is it because they are elderly? Or under the influence of medications that affect their balance? The leaders, physicians and nurses at the San Diego Medical Center considered a range of possibilities and tried everything in the usual playbook, posting pictures of falling leaves on patient doors and using color-coded armbands to indicate fall risk. But nothing was working.
Then the UBT on the 5 West medical-surgical unit cared for a patient who was a member of the facility’s patient advisory council—and they asked his wife for her opinion. She said her husband—normally a self-sufficient, strong man—was too embarrassed to call a nurse to help him to the bathroom, especially given that he was wearing a flimsy, possibly revealing hospital gown.
That “aha” moment led the UBT to take a new approach: No one walks alone. Instead of trying to figure out who is at risk for falling, caregivers would treat everyone as a fall risk and provide assistance. The pilot program was so successful that it is being spread to the entire hospital. Before the campaign began in November 2012, the hospital had been averaging 16 falls a month. In June 2014, that figure was 3.4 a month.
Seeing the experience through the patient’s eyes was the key to the solution.
“I felt as if I was part of the team, and my input was just as valuable as any other member’s,” says Pat, the patient’s wife (last name withheld at her request). “If you go to patients with the attitude that they will be helping you do your job better, you will get an honest evaluation of what can be done to help, and they can make your job easier and more rewarding.”
Sheryl Almendrez, the management co-lead of the Definitive Observation Unit (also called a step-down unit) at the San Diego Medical Center, acknowledges that caregivers on her team were hesitant to have a patient join its improvement work: “They were interested, but were they ready to hear ‘the real truth’?” And what if a chronic complainer ate up valuable time?
As it turns out, there was little to fear. Patients’ requests were reasonable. For example, they want nurses to give them a heads-up when using an ear thermometer. “We’re used to it,” says Almendrez, but they may not know what it is. “They may think it’s an injection coming at them.”
For the Urgent Care unit in Largo, Md., listening to patients’ feedback about long wait times when coming in with a sore throat led that UBT to work with colleagues in the lab to fast-track tests for strep throat.
“Our team was very hesitant about bringing a member in because there could be more complaints than real feedback,” says Donna Fraser, RN, the team’s union co-lead and a member of UFCW Local 400. Making it clear why it was including patients helped: “We told the patient that we want to know what we are doing wrong, because how else will we improve?”
Morales of the Downey NICU says she no longer flinches from criticism, whether or not it’s phrased “constructively.”
“Some of the people we have on our advisory council are the ones who complained the most,” she says. “You know what? They became the advocates for all the other babies. They helped us change a lot of things on our unit for the better.”
Format:
PDF
Size:
38 slides
Intended audience:
UBT co-leads, sponsors, UBT consultants and improvement advisors, especially those working with Level 3 teams
Best used:
Gain tips and tools from three high-performing teams to help your UBT navigate that Path to Performance.
For San Jose Medical Center’s inpatient pharmacy, the road to becoming a high-performing team first required a step—actually a jump—backward.
When the unit-based team was launched in 2010, it quickly was rated at Level 4 on the Path to Performance, the scale for evaluating a team’s effectiveness. The highest level is 5.
“We took it seriously and followed the process,” says Anita Nguyen, inpatient pharmacy director.
Then, in 2012, Nguyen, along with the team’s management and union co-leads, met with UBT consultants to assess their team performance. As they ticked down the list of questions and started to contradict one another, it became painfully clear: They were not the high-performing team they had previously thought.
“As a team we couldn’t answer the questions,” Nguyen says. “It was embarrassing.”
They were knocked down to a Level 1—the most fundamental rating.
Today, the team is a true Level 5, a highly functioning team that recently completed a successful stockroom project to reduce how many drugs are wasted, which is saving more than $10,000 a year. The success is a direct result of opening the department’s budget to the team, which only came about after team members started speaking frankly with one another.
The team’s downgrading was a painful, humbling blow, but most members agree that the assessment was valuable in putting the team on track to do this work and to earning the highest performance rating.
“I was not aware of what a UBT could really do for staff and managers,” Nguyen says. “We recognized the failure and I said, ‘I need you. Let’s work together.’”
Inpatient pharmacy was one of several teams that shared their transformation stories at an event in July at San Jose Medical Center for national Labor Management Partnership leaders. The meeting spotlighted the medical center’s innovative approach to evaluating UBTs and supporting them in delivering the best care possible to Kaiser Permanente members.
Every quarter, San Jose UBT union and management co-leads sit down with their union and management sponsors, and with UBT consultant Heather Williams and Union Partnership Representative Eric Abbott, who support UBTs for the service area. Together they compare the team’s development against the traits outlined in the Path to Performance, including communication among team members and the status of improvement projects. The group then develops a plan for closing gaps, removing barriers and advancing to the next level.
The power of the process is in asking the critical questions, says Joan Mah, the UBT consultant for the San Rafael Medical Center, which has adopted the assessment practice. “Can your team members talk about the metrics? Kinda, sorta? Well if they can’t, we need to connect them with the skills to learn how. The whole point of this is supporting and strengthening. It’s an honest conversation.”
The assessment requires time and commitment from all parties, but by many accounts it is well worth the investment. In addition to San Rafael, which is seeing teams transformed through the process, the approach is being piloted in the Diablo and the Central Valley service areas.
For San Jose inpatient pharmacy, as candid and rigorous as the evaluation process was, it was also invaluable.
“We had to talk about what we really wanted,” says union co-lead Gubatan, an SEIU-UHW steward. “We basically said, ‘Let’s be truthful now. Let’s really do the work.’ ”
The team dramatically improved communication, developed trust, and engaged its members in the journey toward improvement.
“Everyone is empowered to contribute to this process,” Nguyen says. “Before, nobody questioned. Now everyone is empowered to question. With that, people feel like they really belong to the process.”
Format:
PDF
Size:
8.5" x 11"
Intended audience:
Unit-based team members, co-leads, sponsors and consultants
Best used:
This tipsheet suggests ways teams can reach Level 4 or Level 5 in each dimension of the Path to Performance. Post on bulletin boards and discuss in team meetings; use these tips to engage your team in specific actions.