TOOLS
Hank Libs: Easy for You to Say
Format:
PDF
Size:
8.5" x 11"
Intended audience:
Frontline workers and managers
Best used:
Enjoy some variety and fun at a team meeting while highlighting the importance of speaking up.
This short animated video explains how to find and use our powerful how-to guides
Does your team want to improve service? Or clinical quality? If you don't know where to start, check out the team-tested practices on the LMP website. This short video shows you how.
Having trouble using the search function? Check out this short video to help you search like a pro!
Need to find a checklist, template or puzzle? Don't know where to start? Check out this short video to find the tools you need on the LMP website with just a few clicks.
Format:
PDF
Size:
8.5" x 11"
Intended audience:
Frontline workers and managers
Best used:
Enjoy some variety and fun at a team meeting while highlighting the importance of speaking up.
A few months ago, a patient walked from the outpatient clinic to the operating suites at San Francisco Medical Center. He had an infection in his knee that needed to be drained. Paul Preston, MD, was at work and evaluated the man. His condition wasn’t urgent, and he got a bed to wait in.
What happened next is a cautionary tale. The patient’s condition changed—quickly and unexpectedly.
Dr. Preston, who was in charge that day, had moved on and was artfully multitasking on several other matters.
A nurse popped around the corner and interrupted him.
“Dr. Preston, this guy is sick,” she said.
Rapidly changing situations are a part of life in hospitals and clinics. But how they are handled varies wildly, depending largely on whether there is a culture of psychological safety—one where employees can speak up freely and offer suggestions, raise concerns and point out mistakes without fear of negative personal consequences.
Despite volumes of findings linking psychologically unsafe work cultures with poor patient outcomes—up to and including death—the health care industry, including Kaiser Permanente, continues to struggle with creating the culture of open communication that is a key component of safety.
Fortunately, this nurse worked with a physician and in an environment where speaking up is welcomed.
“Boy, was she right,” Dr. Preston recalls. “The patient had become septic in the short time he was there. I was obviously preoccupied, but what she had to say was far more important.”
Positive exchanges like the one that day don’t yet happen reliably enough.
“I think there is a culture of fear around speaking up,” says Doug Bonacum, KP’s vice president of quality, safety and resource management. “We have indication (of that) from People Pulse scores.” In the patient safety world, Bonacum says, it’s still too common to hear of events with adverse outcomes where someone knew something wasn’t right—but didn’t speak up.
Studies have shown that poor communication among surgical team members contributes to a significant increase in patient complications or death (up to four times as many adverse events). Poor communication is also to blame in more than 60 percent of medication errors nationwide.
“If I had a magic wand and could change one thing about the health care culture and the way we work together in order to improve patient care, it would be around our ability to speak up and people's willingness to listen and act,” Bonacum says. “I think it’s mission critical for worker and patient safety.”
Unit-based teams, by addressing issues of status and power, instinctive fear of retaliation and more, are helping build a culture where people are able to speak up. Leaders play a critical role in that transformation by actively developing rapport with employees and/or explicitly admitting mistakes and “disavowing perfection.”
“The definition of leadership is creating the condition to allow your team to succeed,” says Dr. Preston, who is the physician safety educator for The Permanente Medical Group. He notes that in aviation, senior pilots are strongly encouraged to tell those working with them, “If you see anything wrong, please let me know as soon as possible.”
A modified version of that practice, a pre-surgery briefing, now takes place in most Kaiser Permanente operating rooms.
“We don’t really want to say in front of the patient, ‘Hey, if I screw up, let me know,’” Dr. Preston says. “So we go around and say our names and what we’re going to do, and it builds confidence.”
The briefing, he explains, “is a conversation to build the group’s knowledge of what they're supposed to be doing, what to expect and watch out for. It sets the expectation that everyone needs to speak up.”
Dr. Preston says holding a briefing is the single most important thing a surgical team can do for patient safety. And debriefing afterward is critical, too, he says: “It's a chance for teams to consolidate what they learn. . . and get more and more reliable.”
Leaders—physicians, managers, union co-leads and stewards—should model the behavior of speaking up around errors. Creating a blame-free environment, Dr. Preston says, “involves the willingness of leaders to go first in displaying vulnerability. . . by talking about mistakes they made when they wish someone had spoken up.”
Putting in place mechanisms that encourage employees to speak up is another way to foster open communication around errors and performance improvement. Such systems also provide a forum where people learn how to express themselves clearly and non-emotionally—and help to reconnect them with the value and purpose of their work.
South San Francisco Radiology’s unit-based team, for example, has created a structured communication system where radiologic technologists are asked to speak up in the moment and “stop the line” when they encounter anything that deviates from the agreed-upon workflow or is a potential patient safety risk. Afterward, they fill out a brief report that captures the event.
“We made it an obligation for people to speak up,” says radiologic technologist Donna Haynes, the department’s UBT union co-lead and a member of SEIU UHW. “We wanted to empower employees.”
Since implementing the program in April 2012, more than 250 Stop the Line forms have been submitted. As a result, the department has prevented a number of small events from reaching the patient—and has seen a 50 percent reduction of “significant events” from the previous year, incidents in which a patient is incorrectly irradiated, whether it be a wrong body part or a scan is repeated unnecessarily.
The Stop the Line forms are simple and easily accessed in work areas and radiation rooms. They’re not used for punitive purposes; they’re used to track workflow issues that then are addressed by the UBT.
“For us it was a big rush, really trying to empower people to take the time to do what’s right,” says Ann Allen, the medical center’s Radiology director. “Also having trust in the fact that ‘I can submit real data and it will actually implement change.’ ”
Allen’s comment speaks to another huge benefit to creating an environment where people feel free to voice their ideas and concerns: It makes the difference between an organization that is continuously learning and improving performance and one that is stifling innovation and stagnating.
The link between higher-performing unit-based teams and the ability to speak up is clear.
The People Pulse survey has a set of 12 questions that get at a department’s culture and comprise the Work Unit Index. One typical question is, “In my department or work unit, I am encouraged to speak up about errors and mistakes.” In 2011, the survey found that departments where Work Unit Index scores were highest had better HCAHPs scores, more satisfied patients, fewer workplace injuries, lower absenteeism, and fewer hospital-acquired infections and pressure ulcers. Departments whose Work Unit Index scores were in the bottom quartile consistently had poorer performance in those same areas.
“High-performing teams are clear on the goal…and hold each other mutually accountable for outcomes,” Bonacum says. “That level of accountability to each other is what differentiates them and enables people to say something that lower-performing teams can’t and won’t.”
Once you get to a tipping point, Dr. Preston says, people will look out of place if they aren’t speaking up.
“There's no such thing as a perfect day,” Dr. Preston says. Even good surgeons make errors—routinely—and no system, he says, can eliminate human error entirely. “But the earlier the team can recognize what is called an ‘undesired state’ and trap it, the less severe it is. And this is a huge thing for labor and managers, because we’re all there (in the room). Everybody has eyes and ears. The person who’s engaged has a huge role.”
An open, supportive environment is one aspect of a workplace where workers can point out problems when they see them.
But to ensure the support doesn’t evaporate in the stress of a busy day, there needs to be more than the expectation that people will do the right thing. There needs to be a solid system in place that formalizes the commitment to speak up.
A Radiation Oncology team in Northern California knows this firsthand. From the time the South San Francisco Cancer Treatment Center opened in May 2009, its leaders worked to establish a culture that encouraged staff members to speak up when they saw something wrong and to provide input on process improvements. The center didn’t have a clear-cut mechanism for doing this, however; it was fostered through leaders’ encouragement and role modeling.
Then in 2010, a mistake was made—relatively small, but a HIPAA violation: A patient was accidentally given a printout with the personal information of another patient. The member returned the paper to the receptionist, and no lasting harm was done. But it highlighted the fact that staff members needed a way to record process failures, empowering them to address issues large and small, says Marcy A. Kaufman, the center’s Radiation Oncology administrator.
A protocol that calls for submitting a Responsible Report form was already in place for those times when an error reaches the patient. “But we wanted to create something where everyone can give input at all parts of the process,” Kaufman says.
So the unit-based team created what its members call Stop the Line. If a radiation therapist or anyone else in the department encounters anything that deviates from the workflow or compromises care, he or she first acts to ensure patient safety, if such action is needed—and then fills out the Stop the Line form to document the incident. The focus is not on individual error but on what can be done to improve the system to prevent similar mistakes in the future.
“It’s a chance to look at the system to see if it is doing its job—are the checks and balances working? Or do we need to bring to the UBT and come up with a different workflow?” Kaufman says.
At monthly staff meetings, the team pulls out a binder with the Stop the Line reports and discusses the incidents and any follow-up actions taken. That discussion is important not only as a way to close the loop but also because it demonstrates to staff members that their voices were heard. The forms don’t drop into a black hole never to be heard of again.
“You have to constantly be talking about this to keep the momentum going,” Kaufman says.
The process applies to all staff, including physicians.
“In the field of medicine where, in general, it is quite hierarchical, it’s even more imperative we have a system like this to encourage every member of the department to speak up, regardless of title, to make sure we’re giving the best patient care,” says Amy Gillis, MD, the center’s chief of Radiation Oncology.
Dr. Gillis recalled the wrong-patient information episode. The initial assumption was that one of the medical assistants, who normally handle such paperwork, had made the mistake. This time, however, the culprit was a physician.
Staff members hesitated, Dr. Gillis says, wondering, “ ‘Should I really write up a physician?’ ” As she notes, however, “We all need to have a greater awareness.”
“It really does take everyone’s buy-in to make it happen and be successful,” she says. In this case, what it took to convince staff was input from the physicians themselves, with the doctors saying, “Yes, please write that up.”
Stop the Line has been so popular that the cancer center’s four sister centers in Northern California have adopted the practice.
South San Francisco Radiology also adopted the Stop the Line form and process, adapting it to meet its specific needs. The department does hundreds of thousands of scans a year, from mammograms to basic X-rays to CT scans. With such high volume, radiologic technologists often feel pressure to keep patients moving through in a steady flow.
“We needed to give technicians permission to do the right thing,” says radiologic technologist Donna Hayes, the department’s UBT union co-lead and an SEIU UHW member. “We wanted them to know it’s OK to stop the process for this. I think it helped that it also came from management.”
As at the cancer center, the process is not used in a punitive way. Instead, it’s used as a way to highlight and address glitches in the workflow—not only within the department, but also in other departments.
“We’ve been able to take the data back to the orthopedics chief or take ED-related issues back to ED,” says Ann Allen, the Radiology director. “We funnel back to those departments that are partners so they can help us make changes.”
Format:
PDF
Size:
8.5" x 11"
Intended audience:
UBT members, managers, physicians, sponsors
Best used:
Post in working areas and staff break rooms to show that everyone who is a part of Kaiser Permanente can contribute to these three priorities.
Format:
PDF
Size:
8.5” x 11”
Intended audience:
Frontline employees, managers and physicians
Best used:
This poster highlights a Mid-Atlantic States team that reduced patient transport times. Post on bulletin boards, in break rooms and other staff areas.
Format:
PDF
Size:
8.5” x 11”
Intended audience:
Frontline employees, managers and physicians
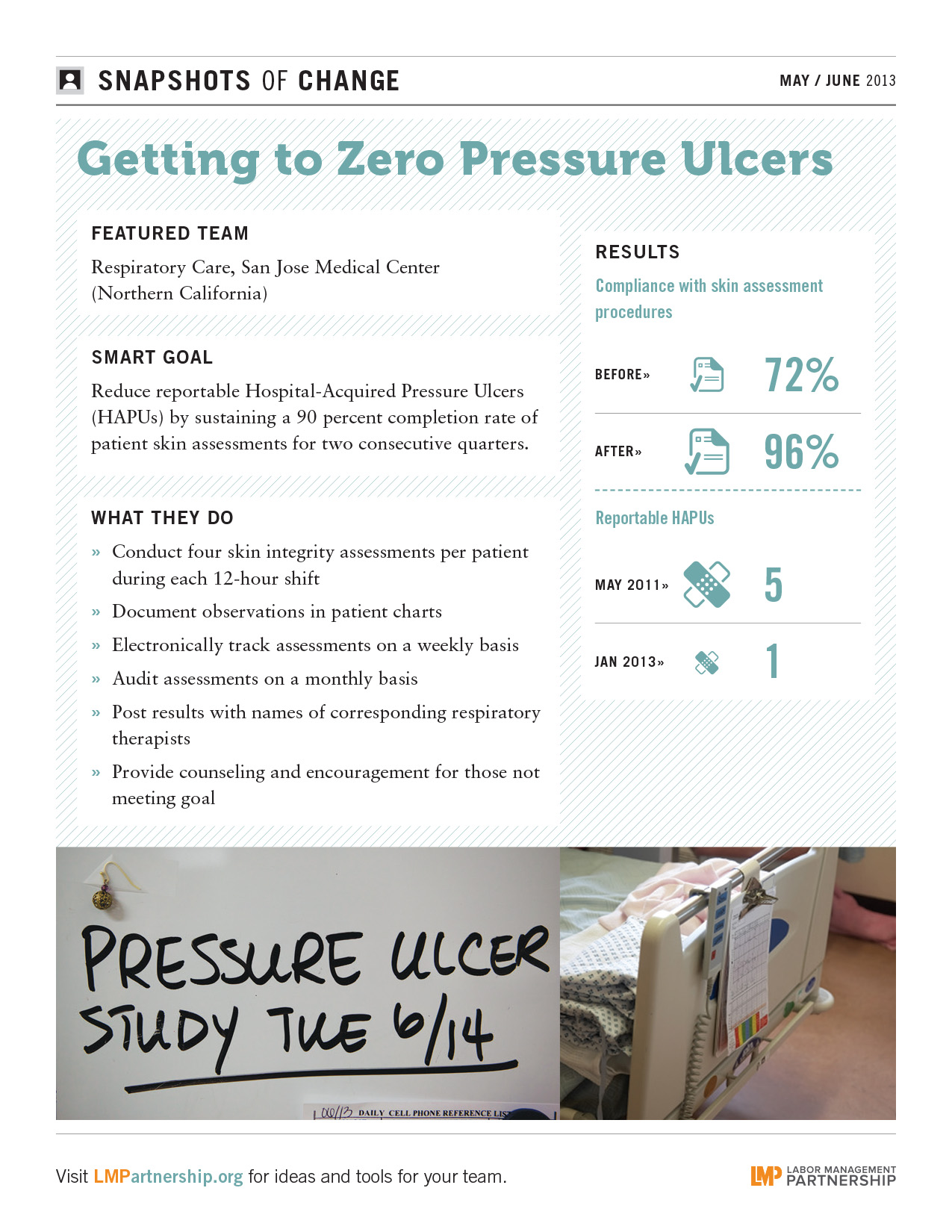
Best used:
Post this in highly visible areas to show your staff how they can reduce pressure ulcers by following a few simple steps.
During the normal stress of being admitted to the hospital, it's not always clear to patients and their families who does what.
And if a nurse or clerk can’t answer a question on admissions, the patient can get frustrated.
So it was in the admitting department at Fremont Medical Center in Northern California, where patients gave low satisfaction scores regarding the process.
“Many different staff use the word ‘admitting,’ so we needed to make sure we stood out, and that patients knew when their admission officially began and ended,” says labor co-lead and admitting representative Joanna Nelson.
Team members thought one of their biggest challenges was making sure patients knew when they were dealing with admitting staff versus other employees.
They first tried using scripted language, the “Right Words at Right Time” (RWRT) approach to let patients know when the actual admission process had started and the representative’s role.
When that failed, the UBT added another level of patient service and rounding, which included a small gift and card.
The gifts were mostly Kaiser Permanente brand items including cups, tablets, aprons, vases or plants. Admitting representatives also gave personal cards to each patient.
“We came up with an extra-special plan for our new admissions. Once the patient was admitted, the Admitting rep went back up to the room—either later that same day or the next day—and gave our patients a welcome gift,” shop steward and OPEIU Local 29 member Nelson says, describing the gesture as a “thank you for choosing our hospital.”
And it worked.
In four quarters, polite and professional customer service scores improved 21 points, and efficient and easy customer service scores picked up three points.
The team also helped by letting patients know how all the pieces fit together.
“Personalize your admitting process,” says Fonda Faye Carlisle, manager, Admitting and Patient Financial Services. “Since the admitting department is not the only voice that says, ‘I will be admitting you,’ admitting needs to personalize so the patient can differentiate between them and others, such as nursing.”
There were team benefits, as well, beyond the scores. Department morale and attendance also increased.
“Our satisfaction is seeing our patients happy and watching our scores improve,” Nelson says.
Department: Adult Medicine, Capitol Hill Medical Center (Mid-Atlantic States)
Value Compass: Service
Problem: Some individual patient transport trips were taking an hour or more, inconveniencing patients and impacting the unit's smooth operation. Staff members sometimes had to wait for a patient to receive medications or had to return to the unit to retrieve a wheelchair adequate for the height and weight of the patient.
SMART goal: Reduce staff time spent transporting a patient by wheelchair from the unit to the lab, pharmacy, hospital entrance or public transit stop from an average of 30 minutes to 15 minutes between May and September 2012.
Union co-lead: Louise Casa, nurse practitioner, UFCW Local 400
Management co-lead: Jacqueline Marshall, RN, clinical operations manager for Adult Medicine
Small tests of change:
Results: Reduced staff time to transport patients from an average of more than 30 minutes to 10 minutes.
A brisk walk by an able-bodied person from the unit to the train station takes about 15 minutes roundtrip—but struggling with an infirm patient in an outdated or inappropriately sized wheelchair could easily double that time.
Other issues included patient dissatisfaction, staff injuries and the added risk of patient treatment delays or falls, says labor co-lead Casa, noting that “we had to look at the problem from many angles.”
The Capitol Hill Medical Center opened with great fanfare in 2011. Hailed as a beacon for affordable and accessible care just as the national debate heated up on these issues, the center attracted attention—and many new members. One key factor that made the new facility so attractive—its proximity to a major public transit station in the District of Columbia—also turned into a potential Achilles heel.
That was until the Adult Medicine UBT rolled in with the right solutions.
The Adult Medicine team started by using performance improvement charting tools to log the time each staff member took to transport a patient to and from the Union Station subway stop or to ancillary departments within the medical center.
The team discovered many of the elderly or wheelchair-using members struggled to make the long trek from the exit doors of Union Station to the waiting room of the Adult Medicine unit, a medical center starting point for most patients.
The team lobbied for new wheelchairs—and for a new transporter position, an OPEIU Local 2 member who transports many of the patients and coordinates the trips that staff members make to the other departments.
In addition, the team now calls ahead to the lab or pharmacy to ensure tests and medications will be ready, or nearly so, when the patient is brought in. It also gives patients red cards to signal their priority status to lab and pharmacy staff.
Format:
Powerpoint
Size:
41 pages
Intended audience:
Frontline employees and managers
Best used:
These slides were presented by three teams that shared their outstanding work on patient safety in a virtual UBT Fair in March, 2013. Use to spread best practices on patient safety.
The teams featured are:
Format:
PDF
Size:
8.5" x 11"
Intended audience:
Frontline employees and teams
Best used:
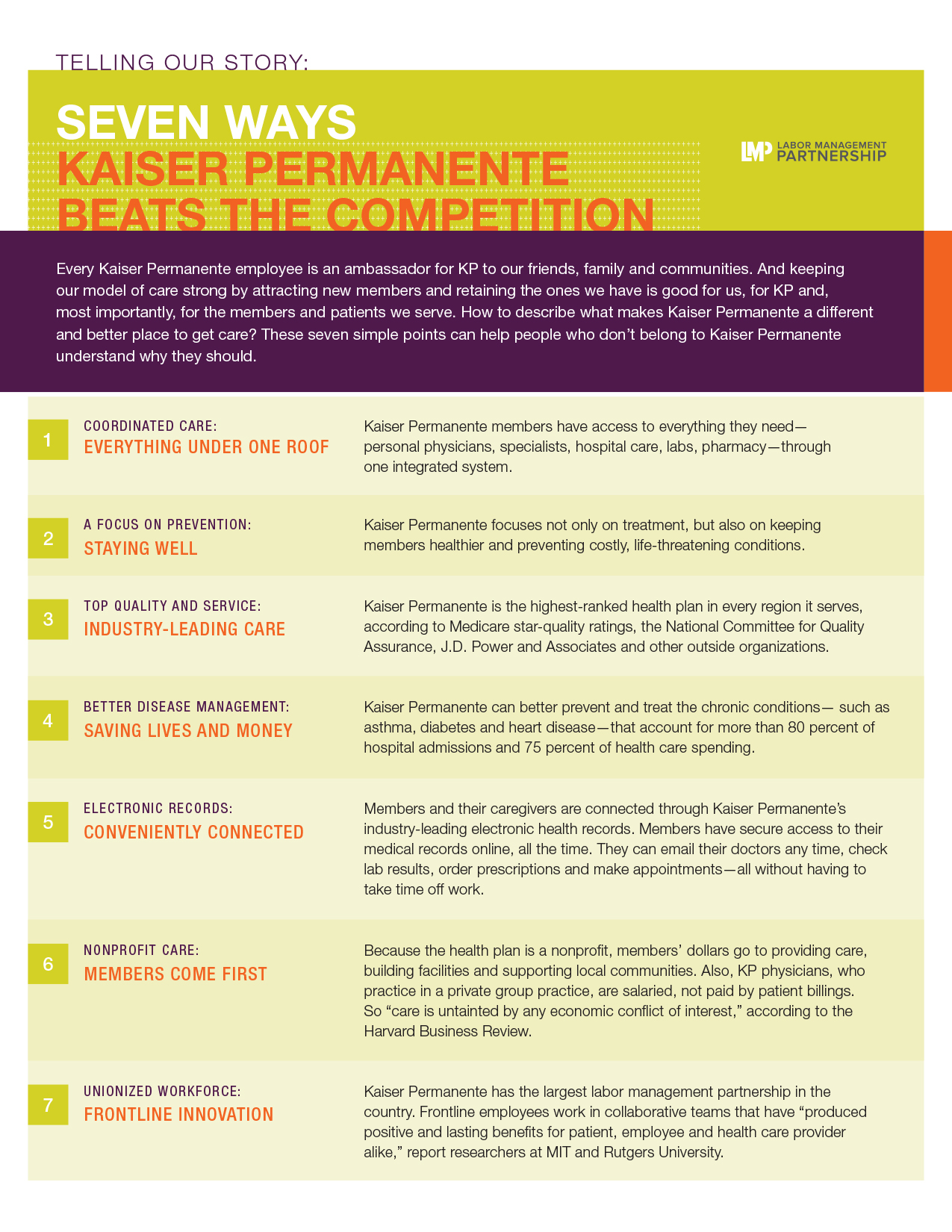
This one-page tipsheet with seven short talking points describes KP's advantages as a health plan. Use to understand how Kaiser Permanente is different and better than other health plans, and to encourge non-members to consider joining KP.