TOOLS
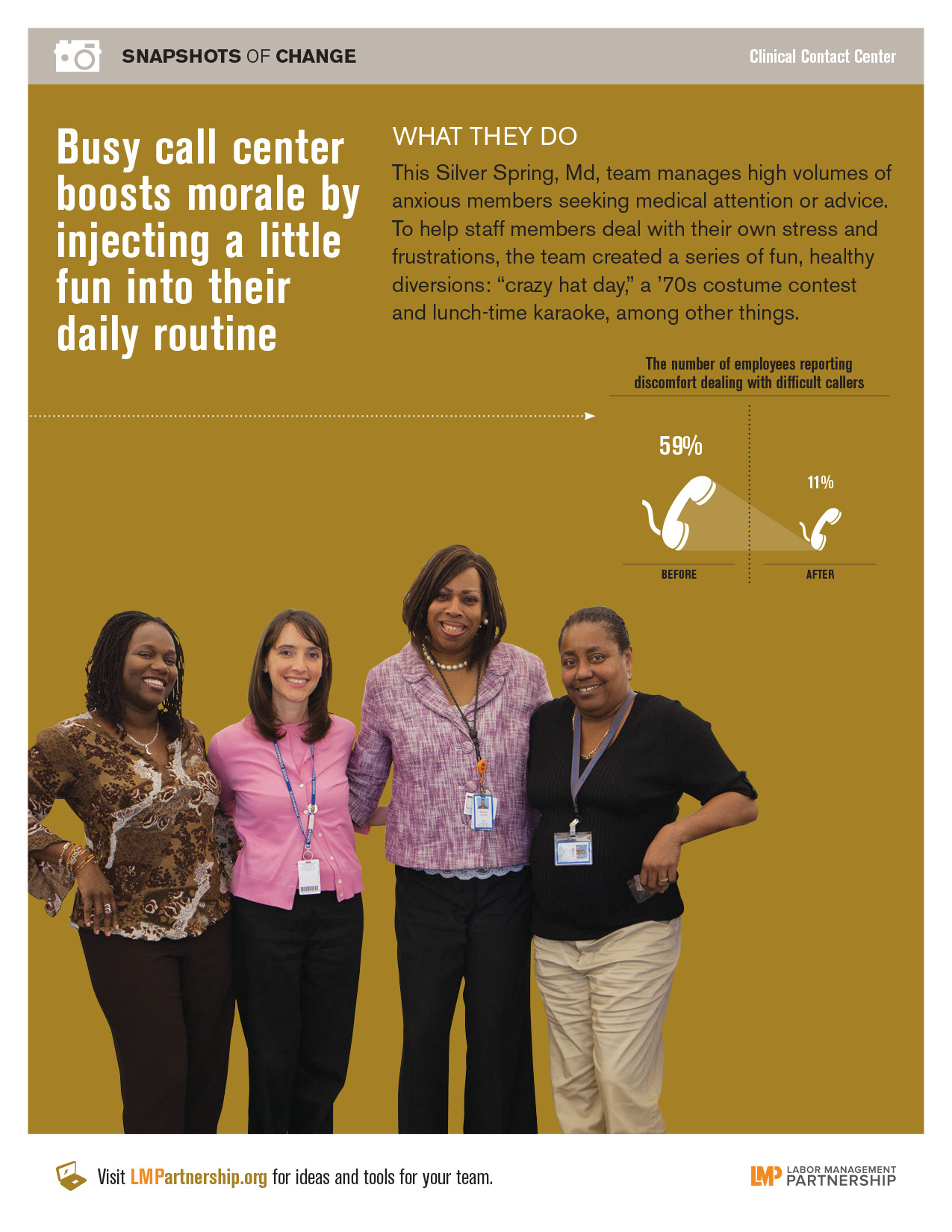
Poster: Busy Call Center Boosts Morale With Fun
Format:
PDF
Size:
8.5" x 11"
Intended audience:
Frontline employees, managers and physicians
Best used:
How can this poster help you and your team find fun ways to boost morale?
This short animated video explains how to find and use our powerful how-to guides
Does your team want to improve service? Or clinical quality? If you don't know where to start, check out the team-tested practices on the LMP website. This short video shows you how.
Having trouble using the search function? Check out this short video to help you search like a pro!
Need to find a checklist, template or puzzle? Don't know where to start? Check out this short video to find the tools you need on the LMP website with just a few clicks.
Format:
PDF
Size:
8.5" x 11"
Intended audience:
Frontline employees, managers and physicians
Best used:
How can this poster help you and your team find fun ways to boost morale?
Format:
PDF (color and black and white)
Size:
8.5" x 11"
Intended audience:
Frontline employees, managers and physicians
Best used:
This poster, for use on bulletin boards in break rooms and other staff areas, highlights an EVS team that uses webinars to spread successful practices.
Amy Edmondson says innovation depends on a culture of focused chaos.
Those words sound like opposites. They are. Don’t worry. It’s not a mistake.
In fact, innovation depends on four pairs of seeming opposites. As unit-based teams ramp up, involving frontline managers, physicians and employees in finding new ways to improve performance and transform health care, they can benefit from creating a culture of innovation. This is how Edmonson, a professor at Harvard Business School, defines the four cultural contradictions of innovation:
Let's take a more detailed look.
“An innovation culture is focused,” says Edmondson. “It is really intent on improving a process or inventing a new business model or coming up with a new product.” At the same time, it is chaotic. “Any idea is welcome and possible—at least until we sort it out. No idea is a bad idea—at least early in the process.”Chaos, says Edmondson, “is about welcoming all ideas, even ‘wacky’ ideas.” Only in a psychologically safe learning environment will employees feel open enough to offer these “wacky” ideas, she adds.
The Labor Management Partnership offers a disciplined process for innovation in the form of the Rapid Improvement Model (RIM) and the plan, do, study, act cycle. But, Edmondson emphasizes, teams use these tools “without knowing in advance what the answer is.” There is a careful and well-managed process, but the content of the conversations about improving performance must be open and inclusive. As teams begin a performance improvement project, UBT leaders need to be very clear about what aspect of performance they are trying to address—not on how the team is going to do it.
An innovative team is one that values those who bring deep expertise (in a specific topic, subject area or clinical specialty, for instance) and people who are broad, general thinkers who span boundaries. “Both of those skill sets are absolutely essential at the same time,” says Edmondson.
In an innovative work culture, “We hold very high standards but we are also very tolerant of failure,” says Edmondson. “That sounds ‘wrong,’ at first,” she admits, “but it is essential because, in innovation, you will never get it right the first time. You try something, test it out, it’s not going to work quite right and then you either tweak it or throw it out altogether and try something else.”
Spreading new ideas that get results throughout a large organization such as Kaiser Permanente, says Edmondson, requires finding ways to “shine a very quiet spotlight”—another seeming contradiction!—on innovators so others become aware of what they are doing and are drawn to try it too.
“In today’s world, there are two ways to get the word out,” she says. The first is face-to-face communication, “positive buzz that starts locally and spreads.” The other is internal online social networks as “a way to listen, motivate and share practices that are potentially better.”
“It can catch on,” says Edmondson. “When there are pockets of effectiveness, other people see them, and they want to play too.”
The theme of the 2012 Union Delegates Conference was “You Gotta Move”—and Amy Edmondson’s advice for the delegates was “you gotta learn.”
The Harvard Business School professor studies what she calls “learning environments.” To support innovation and teamwork, it’s essential the Labor Management Partnership and unit-based teams foster learning environments throughout Kaiser Permanente.
Imagine the ideal learning environment: People feel free to take risks. They feel psychologically safe. They believe they won’t be punished or humiliated for speaking up with ideas, questions, concerns or mistakes. “Without that kind of psychological safety, it’s very hard for an organization to learn,” says Edmondson.
Now imagine the opposite of a learning environment, one where no one speaks up. “Nobody ever got fired for being silent,” says Edmondson. “And yet many bad things happen as a result of silence. Silence is a strategy for individuals to stay safe, but not necessarily for patients to stay safe or for organizations to stay vibrant.”
Creating a learning environment is up to leaders—to those people with influence, whether or not they have a formal leadership role.
“Leaders have to go first,” Edmondson says. They “have to be willing to ask questions themselves, invite participation, acknowledge their own fallibility, and to explicitly state we don’t know everything yet.” These behaviors help an environment where others can take the risks of learning.
But, she cautions, “The learning environment doesn’t live at the ‘organization’ level. For the most part, there are pockets of learning environments.…In a large, complex system, answers don’t come from central headquarters or the CEO. The answers come from the people at the front line doing the work.”
A labor management partnership like the one at Kaiser Permanente “is an important foundation” for building a learning environment, says Edmondson. “A true partnership is completely consistent with the context for mutual learning.”
Both management and union UBT co-leads can help create a learning environment by articulating the unit’s or department’s purpose and goals “in a meaningful way that touches hearts and minds, that motivates and encourages,” she says.
They can—and must—also reduce the fear people experience that makes them reluctant to speak up. The LMP helps develop and support people, helping them be their best and most courageous, Edmondson says.
After Northern California began a regional push in 2009 to improve the identification and diagnosis of malnourished patients, the Roseville Medical Center sought to put the plan to action.
The clinical nutrition team was partifcularly concerned because diet plays a key role in the body’s recovery.
This can be especially true for the elderly and patients with diabetes —two groups at the highest risk for malnutrition. Mary Hart, director of clinical nutrition for Roseville and Sacramento medical centers, says a lack of proper proteins and vitamins affects their ability to recover and heal.
And short hospital stays can be particularly challenging because most patients don’t stay in the hospital very long.
After sifting through the electronic charts of all admitted patients, the dietitians must spot patients “at risk” for malnourishment and reach them in time for a full evaluation and treatment—all before the patient is discharged.
While physicians are the only ones who can make an official diagnosis, they rely on clinical dietitians to assess the patient and alert the physician.
“We keep track of the number of patients who have met the criteria for clinical malnutrition, communicate that to the physician and follow up to see if (the patient) has actually been diagnosed,” Hart says.
The dietitians at Rockville put their assessments and recommendations into a patient’s electronic chart, but everyone did so a little differently.
So they standardized their process and language, which included bolding notes to doctors and speaking directly to them about potentially malnourished patients. Those simple steps made it easier for physicians to know what to look for, and diagnose accordingly.
“It helps because we can see them sooner and start nutritional management sooner and figure out how to refer them to outpatient care after they are discharged,” says labor co-lead and registered dietitian, SEIU UHW, Jennifer Amirali.
The team also piloted a KP HealthConnect tool that made it easier and quicker for clinical dietitians to identify at-risk patients. It pulls data from electronic medical records, and color-codes assessments, recommendations and final diagnoses between dietitians and physicians.
“There was more recognition (among physicians) of what a dietitian does other than just ‘serve food,’” Amirali says.
Hart agreed.
“(Physicians and administration) now see the important role of dietitians in the care team and what we can contribute to the organization and the health of the patient.”
For more about this team's work to share with your team and spark performance improvement ideas, download a poster or powerpoint.
When Helen Bevan told her National Health Services colleagues in the United Kingdom she would be speaking at a conference of Kaiser Permanente union employees, they were surprised.
“What could they possibly learn from us?” they asked.
A lot, she says.
“Kaiser is a role model for us,” explains Bevan, chief of service transformation at the NHS Institute for Innovation and Improvement, part of the largest government-sponsored health care system in the world.“We look at and learn a lot from Kaiser in terms of innovations, efficiencies, use of new technology and its approach to patient care.”
We have much to learn from them as well—especially when it comes to large-scale change.
“To move forward in health care, leaders must tell their story, make it personal, create a sense of ‘us’ and include a call for action,” says Bevan, one of the plenary speakers at this year’s Union Delegates Conference in Hollywood. “The way to build and sustain health care reform is to learn the lessons of social movement leaders.”
Bevan’s point is on the mark. The 700 delegates attending the conference, themed “You Gotta Move,” were called to act on improving their own health and the health of their communities. They took that message to the streets of Hollywood, distributing fliers with tips on easy steps to take to improve health. Some also gathered for a flash mob in front of Hollywood’s Grauman’s Chinese Theatre, dancing to Beyonce’s “Move Your Body”—a song made for Michelle Obama’s “Let’s Move” campaign to end childhood obesity.
“It’s such a great experience to see the extent to which union members are stepping up to be a part of the change process,” Bevan says.
The actions at the delegates conference—and beyond—are precisely what’s needed to reform health care in America and the world, she says, adding: “We can only create large-scale change if we build a platform of commitment and energy.”
Because unit-based teams, KP’s platform for improvement, engage frontline workers, managers and physicians, they “already have that commitment and energy,” Bevan says. UBTs “create a sense of coming together around a common cause and achieving the same outcomes.”
But UBTs alone can’t bring about the large-scale change needed to meet the unprecedented challenges to improve quality and reduce costs.
“Transformation needs to occur at all levels of the organization in order for it to be sustainable,” Bevan says. “Senior leaders need to stop being pacesetters and start engaging, inspiring and emotionally connecting with employees. The passion is there. We just have to tap into it.”
As the task of delivering health and health care becomes more complex and the scale of change increases, “We need to think widely and innovatively about how we define the role of senior leaders,” Bevan says.
That’s where social movement thinking comes in. “Successful movements often have charismatic leaders—think Martin Luther King or Nelson Mandela—but what ultimately guides and mobilizes the movement are leaders at multiple levels.” The key, she says, is to depend less on reorganizing structures and processes as the catalyst for change and more on unleashing emotional and spiritual energy for change.
“People are much more likely to embrace change if it builds on the passion, the sense of a calling that got them into health care in the first place,” Bevan says. By connecting to that shared passion through storytelling, “We can create an unstoppable force for change.”
What happens when things change in your job and you have to rethink what’s always worked in the past?
For me, that moment came two years ago when I moved into a management role. I had spent 24 years as a frontline nurse, union steward and labor partner to hospital administration before my job transition.
Frankly, I wasn’t sure what to expect going in, but having been a steward and a labor partner helped me become a better manager. Kaiser Permanente has given me opportunities to grow as a leader that I don’t believe I would have had elsewhere. Along the way I learned six lessons that I think can help others lead in a collaborative team environment:
As a labor leader, I learned to believe in people and know that there’s always another side to any story. My staff understands they can come to me any time. And our unit-based team helps us draw on everyone’s knowledge and allows everyone to be heard.
In the end, it wasn’t that hard to make the transition from labor leader to manager. In both roles you have to consider diverse points of view, and sometimes you have to step back and ask, “Does it make sense?” You’re not always popular, but I’m OK with that.
We may not always agree. But there is no “we” or “them,” we are all one—because we always put our patients first.
Format:
PDF
Size:
Five pages, 8.5" x 11"
Intended audience:
Frontline teams, managers, senior leaders and physicians, and health care leaders and policy makers
Best used:
Share this Cornell study with teams, colleagues and all parties interested in new approaches to health care delivery and workplace effectiveness—and in learning about the benefits of labor-management partnerships.
Format:
PPT
Size:
1 slide
Intended audience:
LMP staff, UBT consultants, improvement advisers
Best used:
This PowerPoint slide highlights a team that reduced missed antibiotic orders by having two nurses check antibiotic orders. Use in presentations to show some of the methods used and the measurable results being achieved by unit-based teams across Kaiser Permanente.
When your team is on the same page, you all succeed—individually and collectively. By using these team-tested best practices, you can create a proven unit-based team strategy.
Offer frequent refreshers on Consensus Decision Making, Interest-Based Problem Solving, and the Rapid Improvement Model and its plan, do, study, act steps.
Work with your management and union leaders and your facility’s project managers to identify their areas of knowledge and assign them to teams needing that expertise.
Include all the just-in-time, classroom and web-based (KP Learn) courses that meet Path to Performance requirements. Make the list and course-request process easily accessible.
They should sit in on the LMP Council and require regular updates. Identify common issues and address them.
This should be done annually after year-end assessments. Download the tool at LMPartnership.org.
Everyone should be looking to learn on a continual basis.