TOOLS
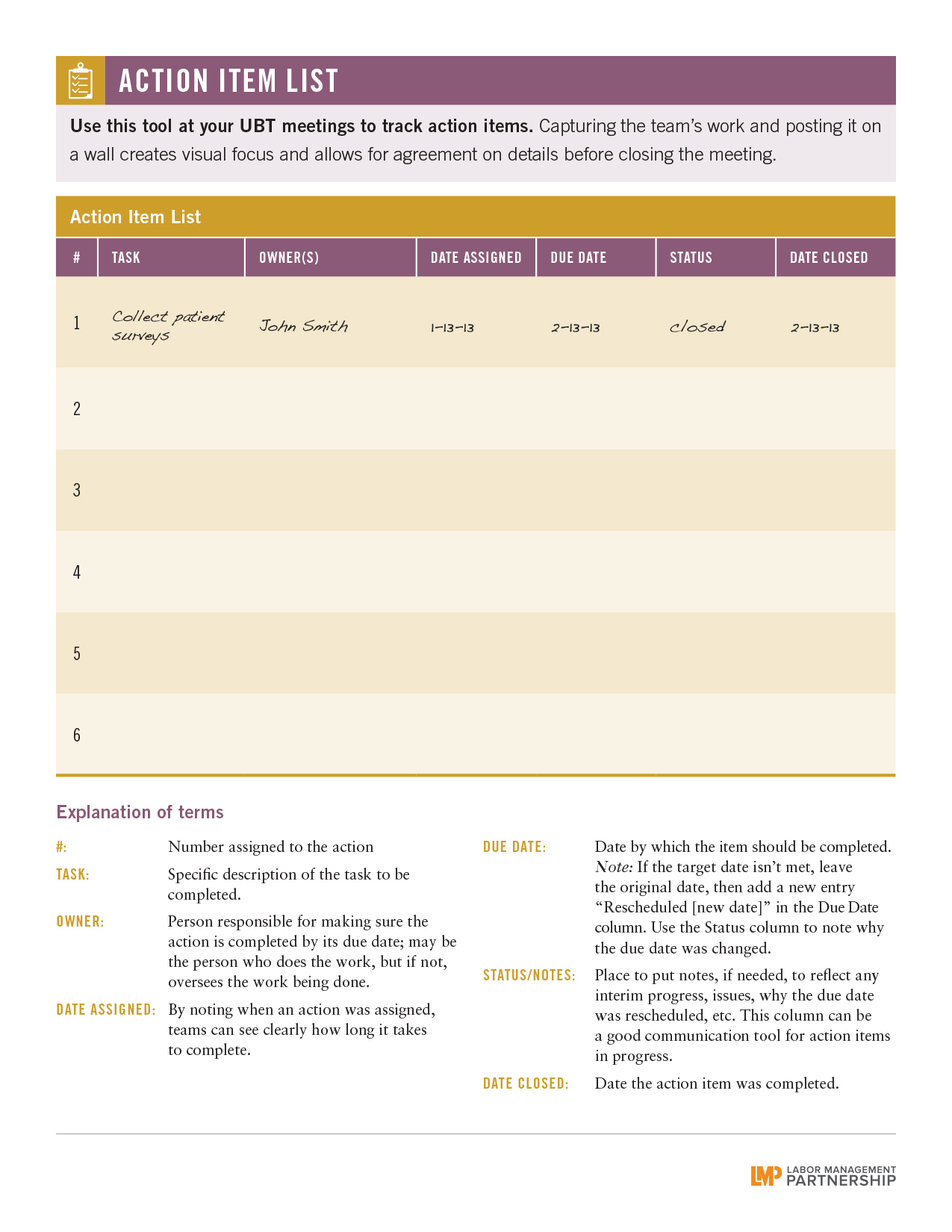
Poster: Action Item List
Format:
PDF
Size:
8.5” x 11”
Intended audience:
Frontline employees, managers and physicians
Best used:
Use this checklist in team meetings to track action items.
This short animated video explains how to find and use our powerful how-to guides
Does your team want to improve service? Or clinical quality? If you don't know where to start, check out the team-tested practices on the LMP website. This short video shows you how.
Having trouble using the search function? Check out this short video to help you search like a pro!
Need to find a checklist, template or puzzle? Don't know where to start? Check out this short video to find the tools you need on the LMP website with just a few clicks.
Format:
PDF
Size:
8.5” x 11”
Intended audience:
Frontline employees, managers and physicians
Best used:
Use this checklist in team meetings to track action items.
Format:
PDF (color and black and white)
Size:
8.5” x 11”
Intended audience:
Frontline employees, managers and physicians
Best used:
Show how you and your staff can get together to make better choices and promote a healthier lifestyle.
See the videos:
When the internal medicine UBT at the Los Angeles Medical Center decided to focus its efforts on African Americans with hypertension, not all team members initially were comfortable with targeting patients by race for special outreach. “We worried about how patients would react,” says union co-lead Marilyn Lansangan.
However, when they invited African-American patients to a special clinic, they were thrilled with the results. Not only did patients show up, the team made progress toward its goal of closing the gap between African-American patients with their hypertension under control and those of other races. “The barrier was not the patients. The barrier was us,” says Lansangan.
Nationwide, nearly 45 percent of African Americans suffer from high blood pressure—a rate much higher than other racial and ethnic groups. The condition tends to develop earlier in life and is likely to be more severe for them. There is some recent research from the National Institutes of Health that suggests genetics may play a part. Such social and economic factors as discrimination and poverty also may contribute. Whatever the reason, health care organizations—including Kaiser Permanente—are working to reduce the disparity.
When Jose Saavedra, M.D., the physician champion on hypertension at LAMC , heard that colleagues at Downey Medical Center held a special outreach clinic for African-American members with high blood pressure, he encouraged the internal medicine UBT to try it as well.
Team members generated a list of their African-American patients with a certain threshold of uncontrolled hypertension. LVNs and social workers called patients every day, inviting them to the special clinic. The success of the outreach calls surprised everyone. “Even when we just left a message, people would come to our clinic,” said Elenita Petrache, assistant administrator and one of the management co-leads.
At the event, clinicians educate patients about hypertension, then take their blood pressure. Depending on the results, patients queue up for a short chat with either a doctor or a nurse, who can adjust their prescription or schedule a more in-depth appointment. Patients who successfully control their blood pressure get a certificate. Everyone gets a swag bag containing an apple, bottle of water, DVD about hypertension, and information about diet and sodium.
Gayle McDow, who attended the clinic in late April, says it make sense for KP to reach out to African-American patients. "The numbers suggest that this issue is more prevalent in our community," she says.
The project also built cohesion among UBT members who work on different floors, says Petrache. “It helped two parts of the department develop a better relationship because we have common goal,” she says. “There is communication between the teams. It’s a beautiful thing.”
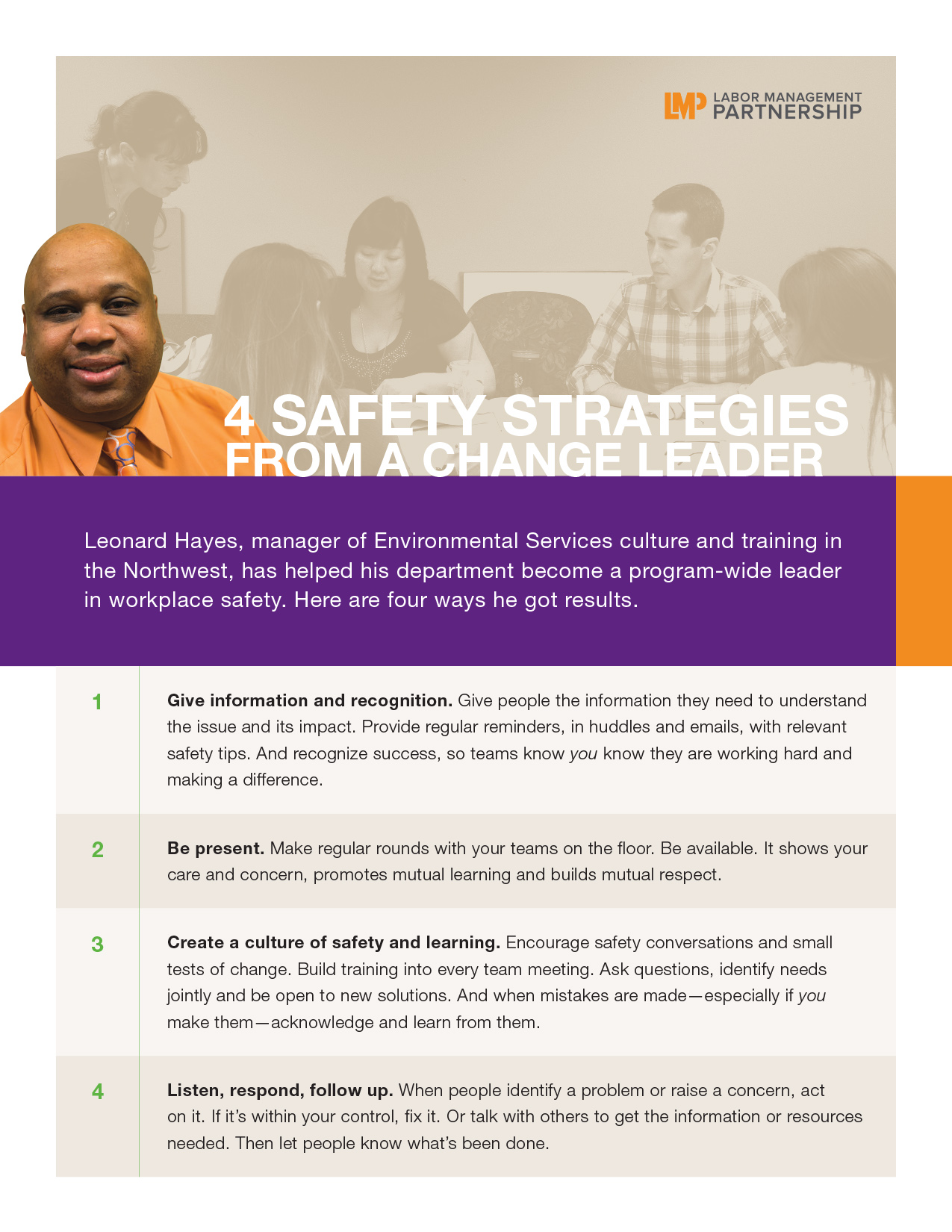
Leonard Hayes, manager of Environmental Services culture and training in the Northwest, oversees workplace safety for 125 outpatient EVS workers in five service areas. This includes the East Side service area, whose EVS unit he directly supervises and which has recorded no injuries for nearly five years. In February 2014, Hayes won the National Workplace Safety Individual Award. He spoke recently with Jennifer Gladwell, LMP communications consultant, about how he engages teams to work more safely.
A. You have to give people information and recognition. Workplace safety is a standing item on our UBT agendas. We talk about working safely, acknowledge how well our teams do and tell them “thank you.” I’ve been put in this job to take away the myths that injuries are inevitable, so people can go home at the end of their shift and enjoy their time outside of KP.
A. I’m in there with them physically. I’ve been a worker and I take interest in what the teams are doing. I try to make sure people know I care for them by being available to them and making sure they have the tools to do their job. I am committed to responding to issues as quickly as possible and resolving them. I have a great labor partner and co-lead, Sherri Pang. She’s been my anchor with the campus and the (East Side) team. She helps me a lot by sending emails, creating fliers, understanding and encouraging the team.
Format:
PDF
Size:
8.5" x 11"
Intended audience:
Managers, supervisors, UBT sponsors
Best used:
These four quick tips from an award-winning manager offer techniques for building a safer workplace.
The Colorado Couriers team is busy with 41 Kaiser Permanente facilities, more than 400 non-KP locations, and about 180,000 pickups and deliveries a year.
When it comes to outside contractors, the SEIU Local 105 contract requires that Human Resources provide the union with specific information about outsourcing, including who is doing the work, the affected job classification, the number of hours involved and what facilities were impacted.
That information wasn’t being provided, so Dominic Jones, a courier driver and Local 105 steward, objected.
“I saw that we were contracting out regular courier service, and it didn’t make any sense,” Jones says. “I knew that it was costing the company more money.”
As a result, the unit-based team took a close look at the department’s processes.
Team members collaborated with couriers in Northern California, who had done similar work, and discovered they could hire another employee, improve routes, reduce use of outside contractors—and still save money.
First steps were to work with internal customers to assess their needs, then reconfigure and bring routes in-house that had been contracted out.
They hired an additional employee to reduce overtime and outside courier costs on the weekends, and purchased new technology for central dispatching that enabled better tracking of pickups and deliveries.
Drivers got smartphones to receive information in real time, which made it possible to monitor drivers’ locations using GPS and find the closest driver for an unscheduled pickup.
In addition to new technology, the team worked with the region’s labs to ensure pickup times met the lab workflow.
“I am very supportive of the work our unit-based team has accomplished,” says Jones, who feels his concerns were addressed by the changes. “We are still outsourcing stat work that we can’t get to, but we are in the process of hiring on-call drivers, which will ease that burden.”
The team exceeded its stretch goal and saved an average of $25,577 a month, a cost reduction of 48.2 percent. By the end of 2013, the team’s effort had resulted in a cost savings of $145,165, and projected a savings of more than $375,000 for the following year.
“We had many painful conversations about how to make this work,” says manager Terry Wagner. “But the team’s input was invaluable. Each individual has been a contributor at some point.”
Sometimes the best way to spread effective practices is to spread experienced people. That’s what happened when the Alpharetta Ob-Gyn UBT in Georgia zoomed from Level 1 to Level 4 in just 10 months after two nurses from two different high-performing UBTs transferred there at the same time.
Jane Baxter and Ingrid Baillie had been UBT co-leads at two different clinics when they each got a new job with the Alpharetta Ob-Gyn department. They both drew on their experiences to guide their new team when they became co-leads at Alpharetta. “We knew the steps in the process and what to expect,” says Baxter, the department’s charge nurse.
Fledgling teams should begin with small performance improvement projects, they say. “We started with the low-hanging fruit,” says Baillie, RN, a member of UFCW Local 1996. “You don’t need to reach for the stars right out of the box.”
And, says Baillie, there’s no need to look any further than Kaiser Permanente’s organization-wide and regional priorities to find plenty of ideas for performance improvement projects—and a wealth of data that is being collected regularly.
“KP makes no secret about what is important to it,” says Baillie. “From that alone, you have all the data you need.”
For instance, the Alpharetta team’s first efforts were to improve clinic start time and get a second blood pressure test for patients with high initial readings. “These are important to KP, and they helped us gel as a team,” says Baillie.
“Small wins help develop confidence,” says Baxter. Now the team is taking on more complex cross-departmental initiatives, such as trying to make available online the big packet of paperwork patients need to complete before a first Ob-Gyn visit.
Getting physicians involved also has been part of this UBT’s success. You won’t find doctors who think UBTs are just for clinic staff on this team, says Baxter.
“Our providers are very invested,” she says. “They take minutes at meetings. We are all on an equal playing field.”
It started with a question from Oncology RN Tom Fought, a member of the Oregon Federation of Nurses and Health Professionals (OFNHP), at the Interstate Medical Office in the Northwest.
Why, he wondered, was primary tubing used for low-reaction drugs instead of the less-expensive short or secondary tubing?
That prompted the department’s unit-based team to start an improvement project that wound up saving $25,000 a year.
When patients come in for chemotherapy or other infusion medications, the drugs are administered via an IV: The bag holding the medication is hung on a pole, with a line that goes into the patient’s vein. When primary tubing is used, the valve to stop the flow of medication is very close to the patient’s body.
If the drugs being used have a high potential for an adverse reaction, it’s essential to use primary tubing, so that if there is an emergency and the line has to be shut, only a very little additional medication reaches the patient.
When the short tubing or secondary tubing is used, the valve to stop the flow of medication is farther from the patient. In this situation, if the valve is closed, more medication is in the line and will flow into the patient until the tube is empty. These types of tubing are appropriate when the medication has a low potential for a negative reaction.
Primary tubing is $4.10 per unit, short tubing is $3.65 and secondary tubing is 65 cents. The costs add up if primary tubing is used when it’s not necessary.
“I had no idea that we would be saving the unit that much money by conforming the tubing,” Fought says.
This team alone was able to save $25,000 a year. If every Kaiser Permanente oncology infusion department adopted this practice, the savings would be dramatic.
“This was such an easy tweak—we just needed to think outside of the box,” says Lacey Anderson, RN, the Infusion Team Lead and a member of OFNHP, who was involved in the project. “The team realized this was such a great idea and wondered, ‘Why haven’t we been doing this all along?’”
Heidi Rolf, the department manager and the UBT’s management co-lead, is proud of the work the team has accomplished. She attributes the success to the leadership of the team and notes that since the team has advanced to a Level 4 on the Path to Performance, team members have more camaraderie and are more engaged.
“At first it was a little difficult to change the habits of the nursing staff,” Fought says. “Within a few weeks, we had everyone on board and our tubing project took off.”
Format:
PDF
Size:
8.5” x 11”
Intended audience:
Frontline employees, managers and physicians
Best used:
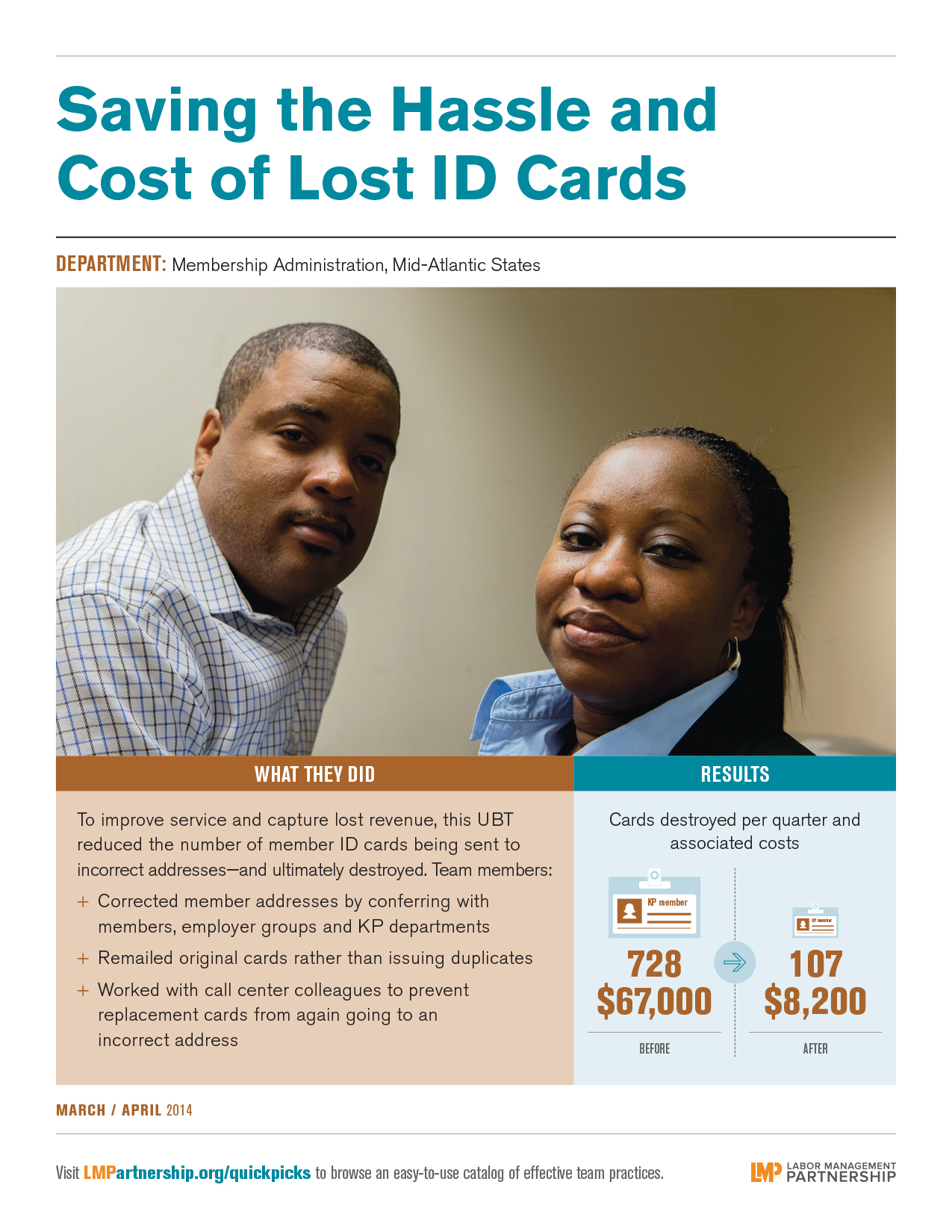
This poster features a Mid-Atlantic States team that has improved service and captured lost revenue. Post on bulletin boards, in break rooms and other staff areas.
The staff at the Radiation Oncology department at the Los Angeles Medical Center knew well the importance of identifying cancer early.
It was part of their clinical routine, and when necessary, they knew patients could begin treatment and slow the spread of the disease.
“We see what happens when you don’t screen regularly,” says Sandra Miller, the department administrator and the UBT’s management co-lead.
So, the UBT was determined to deliver on Kaiser Permanente’s promise of preventive care and leverage the Proactive Office Encounter to increase the percentage of regularly scheduled mammograms, colorectal and Pap screenings by December 2013.
“With Proactive Office Encounter, we are treating the whole member,” says Maria Caceres, an assistant department administrator who was involved with the improvement project.
But the team also had to overcome resistance from patients.
“I think most of our patients that come to us do not want to deal with [one more test],” says union co-lead and medical assistant Monica Villanueva, SEIU UHW. “However, the more we reinforce the importance of having it done, they are more willing.”
Electronic reminders on KP HealthConnect helped ensure patients were getting their screenings, but the team also used a process map to examine its own workflow.
They put color-coded sheets on providers’ keyboards in exam rooms as visual alerts to indicate a patient is due for a screening (pink for mammogram, orange for colorectal test, green for Pap test) and created a pending order in KP HealthConnect.
Medical assistants checked the Proactive Office Encounter before each appointment to alert physicians when screenings were needed, and to check results and make reminder calls to patients.
They gave staff access to the radiology department’s appointment system so appointments could be made for patients while they were in the office, and provided training by laboratory colleagues on how to instruct patients on using the Fecal Immunochemical Test (FIT) kits.
“We had to sit down and break down every step,” Miller says. “We would ask, ‘Where were we not taking advantage of an opportunity to communicate with the doctor or the patient?’ Our process really changed after that.”
As a result colorectal screenings improved by 25 percentage points, Pap smears got a 12-point bump and mammograms increased by 46 points.
And when results for two patients showed they had additional health issues, the physicians, employees and managers were convinced.
“They could see the value and the impact of their hard work,” Caceres says.