TOOLS
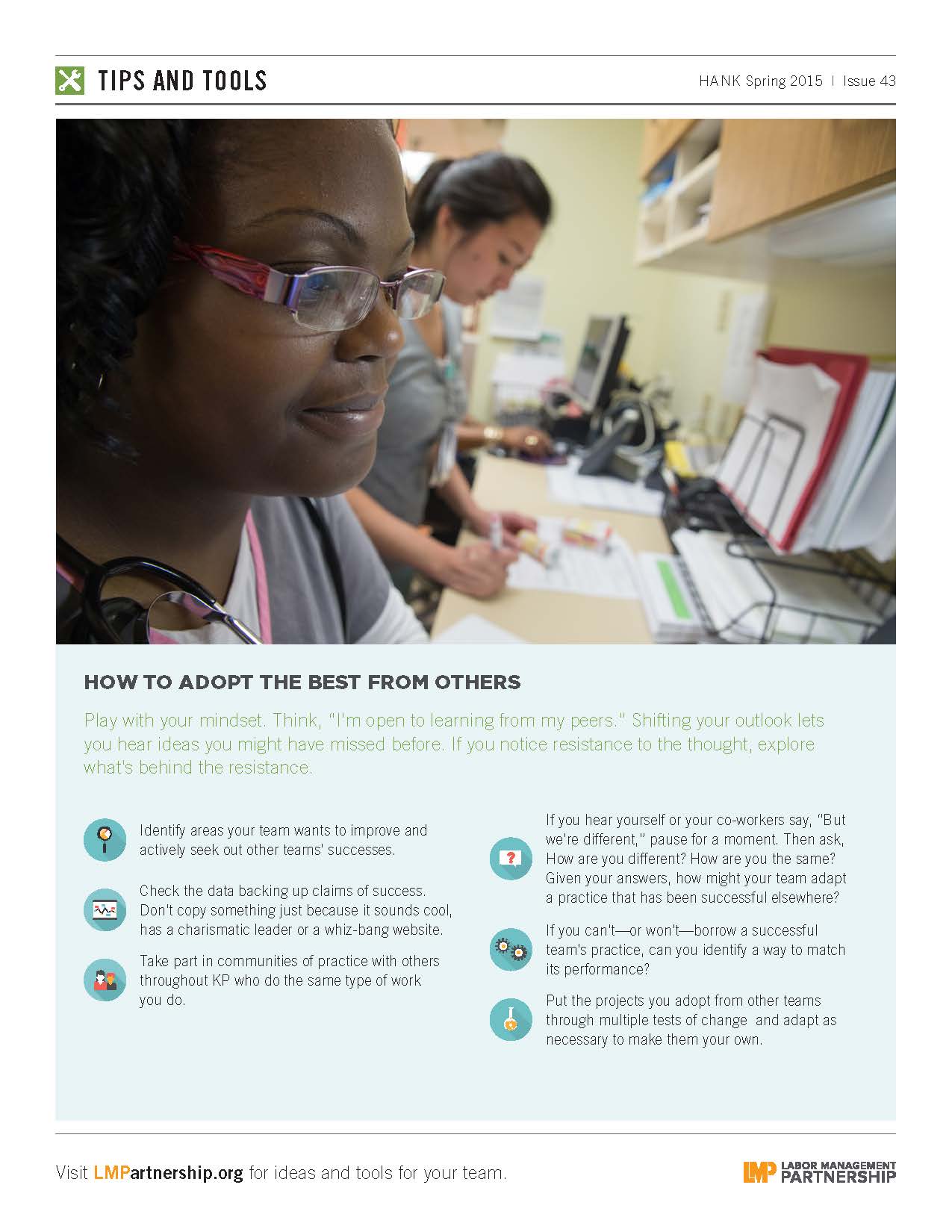
How to Adopt the Best From Others
Format:
PDF
Size:
8.5" x 11"
Intended audience:
UBT consultants and co-leads
Best used:
Get tips on how your team can save time and effort by borrowing successful practices from others.
This short animated video explains how to find and use our powerful how-to guides
Does your team want to improve service? Or clinical quality? If you don't know where to start, check out the team-tested practices on the LMP website. This short video shows you how.
Having trouble using the search function? Check out this short video to help you search like a pro!
Need to find a checklist, template or puzzle? Don't know where to start? Check out this short video to find the tools you need on the LMP website with just a few clicks.
Format:
PDF
Size:
8.5" x 11"
Intended audience:
UBT consultants and co-leads
Best used:
Get tips on how your team can save time and effort by borrowing successful practices from others.
Format:
PDF
Size:
8.5" x 11"
Intended audience:
UBT consultants, co-leads and Sponsors.
Best used:
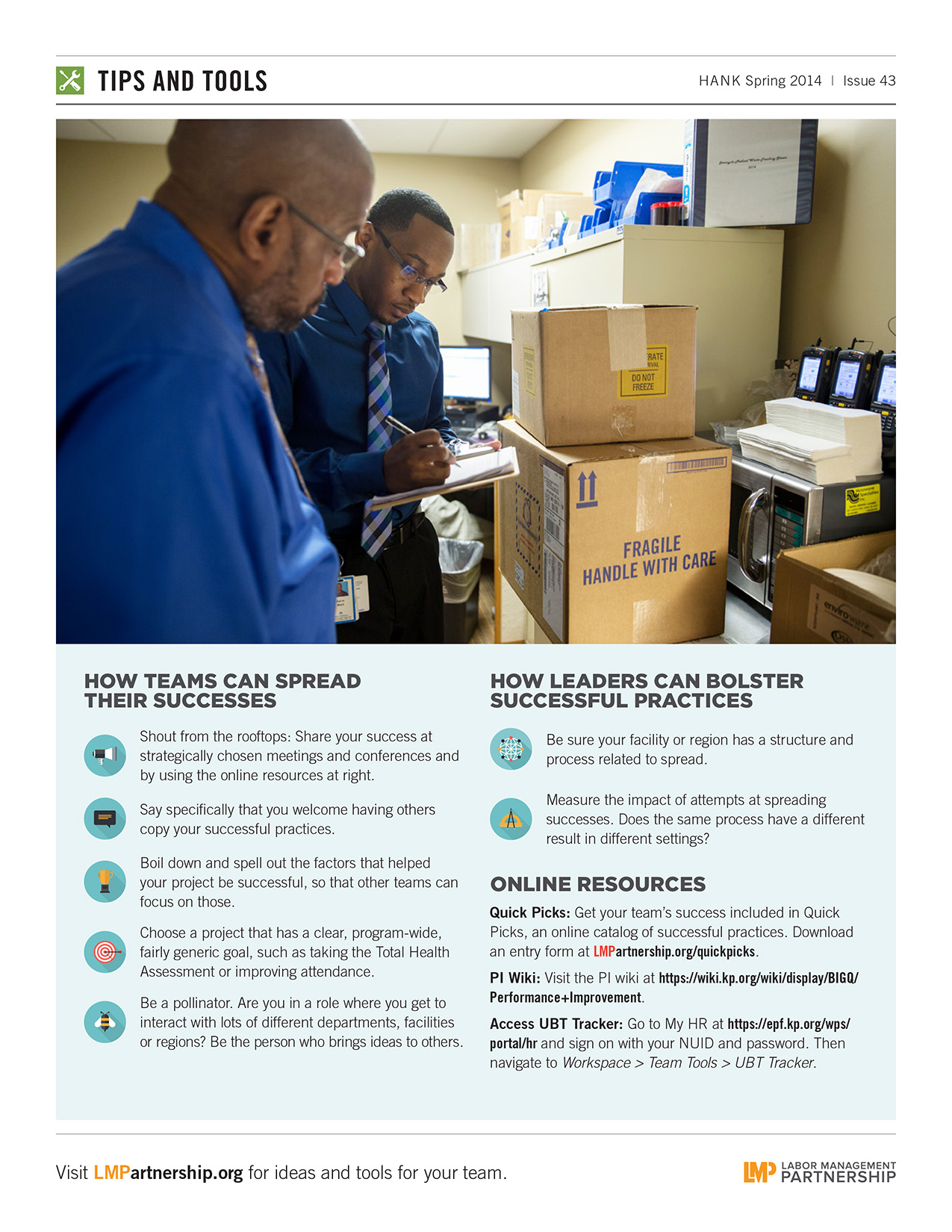
If your team has developed a great practice that others could benefit from, use this tool to see how you can spread it throughout your facility and beyond.
Format: PDF
Size: 8.5" x 11"
Intended audience: Frontline workers, managers and physicians who enjoy a bit of humor
Best used: Post in your workspace or in a team breakroom to remind everyone that borrowing good ideas is a great practice!
Description: This cartoon first appeared in the Spring 2015 issue of Hank.
(3:28)
In this short video, see how the Neo-Natal Intensive Care Unit at Kaiser Permanente's Downey Medical Center is turning parents' ideas for improvements into reality.
Format:
PDF (color and black and white)
Size:
8.5” x 11”
Intended audience:
Frontline employees, managers and physicians
Best used:
Post on bulletin boards, in break rooms and in other staff areas, and use as a discussion tool during meetings to remind your team members we embrace a culture of openness.
Format:
PDF
Size:
8.5” x 11”
Intended audience:
Frontline employees
Best used:
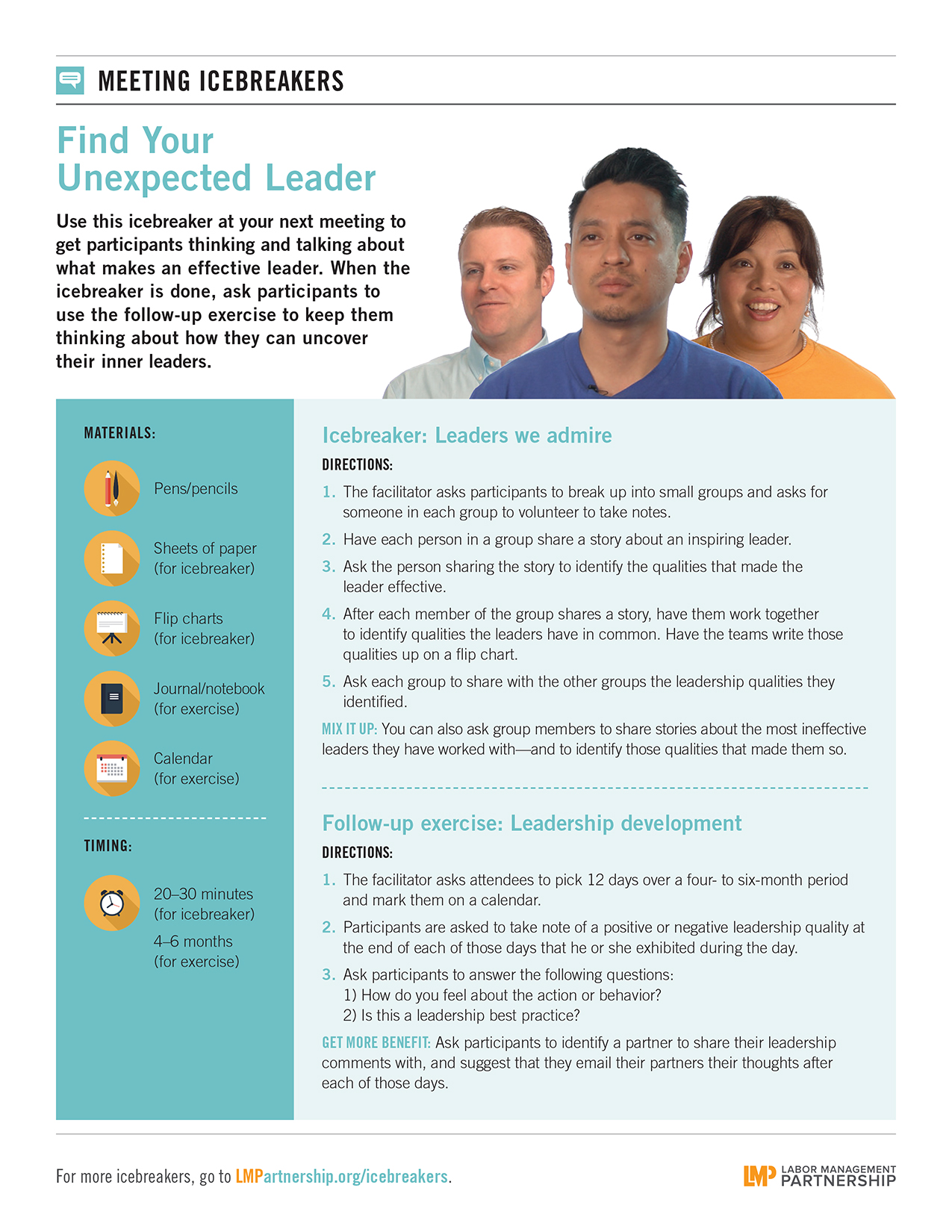
After showing the LMP video "Find Your Unexpected Leader" at your next meeting, use this icebreaker and follow-up exercise to get participants thinking and talking about what makes an effective leader.
Fists pounding on tables, demands, showdowns, strikes. So went traditional collective bargaining: Each side fighting for a bigger slice of the same pie. Each side gunning for a narrowly drawn agreement on pay and working conditions, leaving mutual concerns about patient care, quality and affordability unaddressed.
But Kaiser Permanente and the Coalition of Kaiser Permanente Unions abandoned the traditional approach in 1997, when they founded the Labor Management Partnership.
Our negotiations feature committees, observers and flip charts of options. Since 2000, KP workers, managers and physicians have worked together to craft four National Agreements and one reopener amid relative labor peace. On March 30, some 150 representatives will begin to negotiate a fifth agreement. Assuming all goes according to schedule, the new contract for the 100,000 workers represented by 28 locals in the coalition will be ready to go into effect when the 2012 National Agreement expires Sept. 30.
In an age of growing health care costs and increased competition, the joint goal is to provide our health plan members and patients with better, faster, less expensive and more personal care and to maintain and improve the best health care jobs in the United States.
“Interest-based bargaining is not a utopia and not always a win-win. It’s taken Kaiser and the unions a lot of hard work to get where they are,” says Linda Gonzales, director of mediation services for the Federal Mediation and Conciliation Service, Southwest Region. “[But] to resolve difficult issues in partnership is a strength.”
Because of interest-based bargaining, Kaiser Permanente and the Coalition of KP Unions have been able to go well beyond wages and benefits—the subjects of traditional bargaining—in negotiating four program-wide contracts. These National Agreements have developed industry-leading approaches to worker sick leave, safety and training and workforce development. They have created unit-based teams to improve patient care and service, set standards to hold teams and their sponsors accountable, and pioneered programs for the mutual growth of KP and the unions.
Interest-based bargaining pays off in other ways as well.
“To understand one another’s interests, you have to engage in inquiry and listening, and you have to resist jumping to conclusions about the other party’s intentions,” says Harvard Business School Professor Amy Edmondson. “Doing this develops leaders who better understand how the organization works.”
“People in health care look to Kaiser Permanente as the showcase for working together,” says Gonzales, who helped facilitate bargaining for the first National Agreement in 2000.
The mediation service last year recognized a handful of cases of successful interest-based bargaining. Our Labor Management Partnership was one of them.
Picture a large room with 150 people. Hands are raised. Everyone gets heard. It is pushing midnight and exhaustion is setting in, but everyone maintains a sense of mutual respect and serious purpose.
It’s not the United Nations but the Common Issues Committee (CIC). The CIC is a representative group—made up of Kaiser Permanente workers, managers and physicians as well as delegates from the Coalition of Kaiser Permanente Unions—who take on the responsibility of negotiating a new National Agreement. The program-wide labor contract covers the 28 locals in the union coalition.
This inclusion is part of what makes our negotiations different from other labor contract negotiations—because how we bargain greatly affects what we bargain. By seating RNs and regional health plan presidents with lab techs and program managers during negotiations, interest-based bargaining at KP opens up new issues for discussion and creates deeper support for the final agreement.
“I personally learned a lot from the different perspectives voiced by all of the individuals representing their fields,” says Dr. Varoujan Altebarmakian, a medical group representative on the 2012 CIC. What he learned during bargaining, he says, made him an even more active advocate for partnership at Fresno Medical Center, where he is physician-in-chief.
A new CIC is formed each bargaining year. KP and union leaders select members and assign each to a subgroup to address a topic area. This year, those topics are expected to include Total Health, Work of the Future, and Operational and Service Excellence in Partnership.
Each subgroup is co-led by a management and union representative. Instead of taking hard-line positions, subgroup members stake out their common interests. Over the course of five bargaining sessions, assisted by outside facilitators, they identify interests and develop options.
In 2010, that process led to development of the Path to Performance, which established a uniform way of rating UBTs. “It was a defining moment in partnership,” says LaMont Stone, a labor liaison for Local 29 in Northern California who participated in 2010 and 2012 bargaining. “Before it was case by case, region by region.”
At the final bargaining session, each subgroup brings its proposals to the full CIC for discussion and agreement; the full CIC also negotiates wages and benefits. The finalized contract then goes to KP management for approval and is ratified by the members of each local in the union coalition.
Each day, more than 3,500 unit-based teams use interest-based problem solving and consensus decision making to improve performance and resolve issues throughout Kaiser Permanente. Those same techniques guide negotiations for the National Agreement.
The interest-based process differs from traditional bargaining in several ways. The first major difference can be seen in the room, says Dawn Bading, vice president of human resources for the Georgia region.
“The way we physically sit is different,” she says. “In traditional bargaining, labor sits on one side and management sits on the other. With interest-based bargaining, we sit at a U-shaped table and we are interspersed together. Beside me may be a union rep and on the other side may be someone from management. This physically represents the interweaving of thoughts and ideas.”
This intermingling continues as the negotiations begin, says LaMont Stone, labor liaison for OPEIU Local 29 in Northern California.
“In regular bargaining, you start apart and try to come together,” says Stone, who has participated in bargaining the last two National Agreements. “Here, we start together and try to stay together.”
Part of the power of interest-based bargaining is that in the early stages, the parties aren’t staking out possible solutions.
Walter Allen, executive director and CFO of OPEIU Local 30, says that in traditional bargaining, sides may start off with extreme positions to better their chances of getting what they actually want in the negotiations. “I’ve heard some unbelievable proposals, such as having Groundhog Day off,” Allen says. “Because we don’t do proposals (positions)—we do interests—you don’t get that here. You have to say why this is an interest. How can you argue seriously for Groundhog Day off? No one wants to defend a stupid proposal. Interest-based bargaining eliminates a lot of nonsense.”
This step also helps each side see how much they have in common before moving on to develop options and reach consensus.
“At times it was tedious,” says Angela Young, a unit assistant at Roseville Medical Center. An SEIU-UHW member, Young was a 2010 and 2012 member of the Common Issues Committee and is headed to bargaining again in 2015. “But it keeps the conversation going, and got us where we needed to be. That’s a good thing.”